Published: March 2013
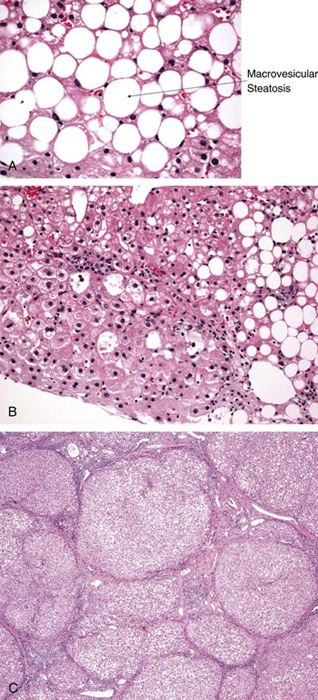
Nonalcoholic fatty liver disease (NAFLD) is one of the most common causes of chronic liver disease. It encompasses a spectrum of conditions associated with lipid deposition in hepatocytes. It ranges from steatosis (simple fatty liver), to nonalcoholic steatohepatitis (NASH–fatty changes with inflammation and hepatocellular injury or fibrosis), to advanced fibrosis and cirrhosis (Figure 1). Studies suggest that although simple fatty liver is a benign condition, NASH can progress to fibrosis and lead to end-stage liver disease. The disease is mostly silent and is often discovered through incidentally elevated liver enzyme levels. It is strongly associated with obesity and insulin resistance and is currently considered by many as the hepatic component of the metabolic syndrome. NASH cirrhosis is now one of the leading indications for liver transplantation in the United States.
Because NAFLD resembles alcoholic liver disease but occurs in people who drink little or no alcohol, excessive daily alcohol consumption must be ruled out before making the diagnosis. Numerous other conditions leading to fatty liver must be excluded by history, physical examination, and appropriate testing (Table 1).
Accurate epidemiologic data are not available because of a lack of population-based studies and reliable noninvasive screening tools. There is disagreement about the methods used to diagnose NASH, and there is no clear consensus on the clinical implications of histologic changes or on the influence of the amount of alcohol ingested. The prevalence of NAFLD is affected by many factors, including genetics (predilection to alcohol abuse, sex) and environment and is therefore difficult to define. In general, the risk of liver disease increases with the patient's body mass.
Based on the available data, NAFLD is estimated to occur in one-third of the general population in the US. The prevalence of NASH is more difficult to determine. It seems to occur in approximately 3% of the US population but may be found in more than 25% of obese persons.
The prevalence of overweight persons (body mass index [BMI] ≥25 kg/m2) in the US has risen to more than 65%, and obesity (BMI ≥30 kg/m2) is now present in more than 30% of the adult US population. The prevalence is increased in men, older individuals (those aged 40-70 years), and those with components of the metabolic syndrome especially diabetes and abdominal obesity. The prevalence of childhood obesity and NAFLD is at similar levels. NAFLD has been observed in all ethnic groups with the highest prevalence seen in Hispanics compared with Caucasians and African Americans.
| Nonalcoholic fatty liver disease |
|---|
| Excessive alcohol consumption |
Drugs
|
| Hepatitis C (genotype 3) |
Nutritional factors
|
Surgical considerations
|
Metabolic disorders
|
Syndromes associated with obesity and insulin resistance
|
Other
|
Copyright © 2013 The Cleveland Clinic Foundation.
Development of NASH may be the result of 2 liver insults. With the initial insult, macrovesicular steatosis occurs which is a manifestation of excessive triglyceride accumulation in the liver. Insulin resistance and subsequent hyperinsulinemia appear to lead to alterations in the hepatic pathways of uptake, synthesis, degradation, and secretion of free fatty acids and ultimately to accumulation of lipids in the hepatocytes. These changes seem to make the liver susceptible to a second insult, resulting in an inflammatory response and progression of liver damage. Oxidative stress, mainly caused by mitochondrial dysfunction, and proinflammatory cytokines such as tumor necrosis factor-alpha (TNF-alpha), are believed to play an important role in the progression of liver damage in NAFLD. Potential oxidative stressors include hepatic iron, leptin, antioxidant deficiencies, and intestinal bacteria. Hepatocyte apoptosis, an organized form of cell death, has been identified as a potential key component of the second insult involved in NAFLD progression.
Overall, morbidity and mortality have been shown to be significantly higher in NASH patients compared with the general population. Coronary artery disease and malignancy followed by liver-related mortality are the most common causes of death in NASH patients. Children with NASH also have a significantly shorter duration of survival compared with people in the general population. Data suggest that the natural history of NAFLD is determined by the severity of the histologic damage. Most patients with NAFLD have pure steatosis without inflammation and are reported to have a benign clinical course. Of patients with NASH 15% to 25% progress to cirrhosis and its complications over 10 to 20 years. At the time of initial biopsy, as many as one-third of NASH patients have advanced hepatic fibrosis, whereas 10% to 15% have well-established cirrhosis. It is now recognized that a large portion of patients with cryptogenic cirrhosis have burned-out NASH: the histologic feature of steatosis or steatohepatitis is replaced by a bland cirrhosis. NASH cirrhosis is a risk factor for development of hepatocellular carcinoma (HCC). Some studies report a prevalence of HCC in NAFLD patients of 0% to 0.5% and 0% to 2.8% in NASH patients over a 20-year period. Data in Japanese patients suggest that the cumulative rate of HCC at 5 years may be as high as 15%. NASH-associated cirrhosis is an increasing indication for liver transplantation. Recurrence after liver transplantation has also been reported as has de novo NAFLD following liver transplantation for other reasons.
Further studies are needed to define the pathogenesis of NAFLD clearly and explain the apparent inter-individual variation in the susceptibility to progress to more-advanced liver disease. Genetic factors have been suggested to play an important role in this variation, and several new candidate genes have been proposed.
Most persons with NAFLD are asymptomatic, and liver disease is often discovered incidentally when laboratory examination shows elevated liver enzyme levels. It is the most common cause of unexplained persistent elevation of liver enzyme levels after hepatitis and other chronic liver diseases have been excluded. The most common symptoms that bring NAFLD to medical attention are malaise, fatigue, and right upper quadrant or diffuse abdominal discomfort. Hepatomegaly is commonly found on clinical examination. When cirrhosis appears, stigmata of chronic liver disease, such as spider angiomata, ascites, splenomegaly, hard liver border, palmar erythema, or asterixis, can be present. Patients might complain of jaundice or pruritus, or they might present with a complication of portal hypertension (eg, ascites, variceal bleeding, or encephalopathy). Most patients have associated features of the metabolic syndrome (Table 2): obesity (47%-90%), diabetes mellitus (28%-55%), and variable incidences of hyperlipidemia (4%-92%) and hypertension.
| Parameter* | Value |
|---|---|
| Impaired glucose tolerance | Fasting blood glucose level ≥110 mg/dL |
| High blood pressure | ≥130/85 mm Hg |
| Elevated triglyceride levels | >250 mg/dL |
| Low high-density lipoprotein level | <40 mg/dL for men; <50 mg/dL for women |
| Abdominal obesity | Waist: >102 cm (40 inches) for men; >88 cm (35 inches) for women |
* Metabolic syndrome is diagnosed by the presence of 2 or more of these parameters.
© 2013 The Cleveland Clinic Foundation.
NAFLD is usually diagnosed during further evaluation for elevated aminotransferase levels found in one of three situations: on routine checkup, when monitoring is performed for possible side effects of drugs (most often cholesterol-lowering medication), or for nonspecific symptoms. NAFLD can also be identified incidentally on imaging or, less often, on liver biopsy done for other reasons. Some centers screen for NAFLD in high-risk groups that include patients with elements of the metabolic syndrome.
Clinical evaluation includes a careful history and physical examination. It is particularly relevant to inquire about excess alcohol consumption—defined as >30 g/day for men and >20 g/day for women within the past 5 years; 350 mL (12 oz) of beer, 120 mL (4 oz) of wine, and 45 mL (1.5 oz) of hard liquor each contain 10 g of alcohol—and to define the nonalcoholic nature of the condition. Moreover, it is necessary to exclude the alternative causes of fatty liver (Table 1). It is most important to include anti-hepatitis C antibody as well as serum ceruloplasmin levels in young patients.
Primary noninvasive evaluation may be used to confirm the diagnosis of fatty liver disease, given the risks and costs of a liver biopsy. Clinical factors and basic laboratory evaluation, particularly in patients aged 45 years and older, or those with obesity, type 2 diabetes mellitus, or an aspartate aminotransferase-to-alanine aminotransferase (AST/ALT) ratio >1, have been shown to be predictors of more-severe histologic disease and may be useful in making a decision regarding when to order a biopsy. Histologic evaluation is the gold standard and should be considered.
In a patient with suspected NAFLD or NASH, useful baseline testing should include levels of AST, ALT, total and direct bilirubin, and fasting serum glucose, as well as a lipid panel. Mild to moderate elevation of serum aminotransferase levels is most commonly found (mean range, 100-200 IU/L). Generally, the ratio of AST to ALT is <1, but this ratio increases as fibrosis advances. Liver enzyme levels are normal in a large percentage of patients with NAFLD; normal aminotransaminase levels do not exclude the presence of advanced disease. Serum alkaline phosphatase and g-glutamyl transpeptidase levels may also be mildly abnormal. Given that more than 80% of patients with NAFLD have some components of metabolic syndrome, serum levels of fasting cholesterol and triglycerides, as well as fasting glucose and insulin, should be determined. Albumin, bilirubin, and platelet levels are usually normal unless the disease has evolved to cirrhosis. Some patients with NAFLD have low titers of autoimmune antibodies (antinuclear and anti–smooth muscle antibody) and an elevation of ferritin. The role of these markers is still unclear.
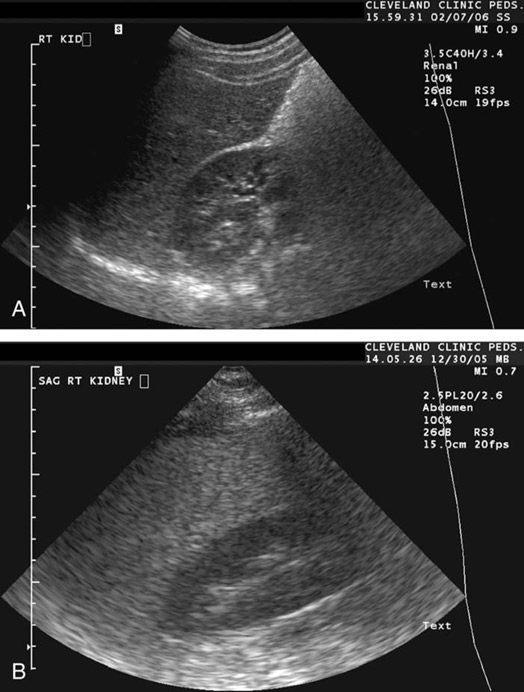
A liver ultrasound examination is useful for confirming steatosis. Fatty infiltration of the liver produces a diffuse increase in echogenicity (a bright liver) and vascular blurring (Figure 2). Unfortunately, ultrasound cannot rule out steatohepatitis or fibrosis, and its sensitivity drops sharply when <30% of hepatocytes contain fat droplets. It also has low accuracy in obese patients. Both computed tomography (CT) and magnetic resonance imaging (MRI) studies, especially the new technique of magnetic resonance spectroscopy, are more sensitive modalities for quantifying steatosis. However, none of these imaging techniques has sufficient sensitivity and specificity for staging the disease and cannot distinguish between simple bland steatosis and NASH with or without fibrosis. Hepatic elastography is a non-invasive measurement of hepatic fibrosis by measuring liver stiffness, which is increased with increased fibrosis. Ultrasound elastography is limited in obese patients. Magnetic resonance elastography has not been shown to detect NAFLD. Elastography is currently not widely available in the US.
Liver biopsy is of unquestioned value in determining the presence of steatosis, distinguishing steatosis from steatohepatitis, and assessing the degree of fibrosis. Because the diagnostic accuracy of noninvasive diagnostic tools is low, histology is the most reliable means to grade the severity of the disease and thus estimate prognosis. Biopsy is also helpful in ruling out an alternative diagnosis. In addition to establishing the cause and severity of disease, histology permits the monitoring of disease progression and the response to therapy, because aminotransaminase levels can decrease during the course of the disease regardless of whether fibrosis progresses or improves. A histologic scoring system (NAFLD activity score) has been proposed to aid with diagnosis and monitoring of the disease.
NAFLD is histologically indistinguishable from liver damage resulting from alcohol-induced liver injury. The steatosis seen in NAFLD is macrovesicular. In adults, similar histologic findings can be found in a number of conditions (Table 1). The spectrum of abnormalities varies from simple bland steatosis to NASH, in which steatosis is associated with mixed inflammatory cell infiltration and liver injury. Cell injury is manifested by hepatocyte ballooning and by Mallory hyaline and acidophil bodies.
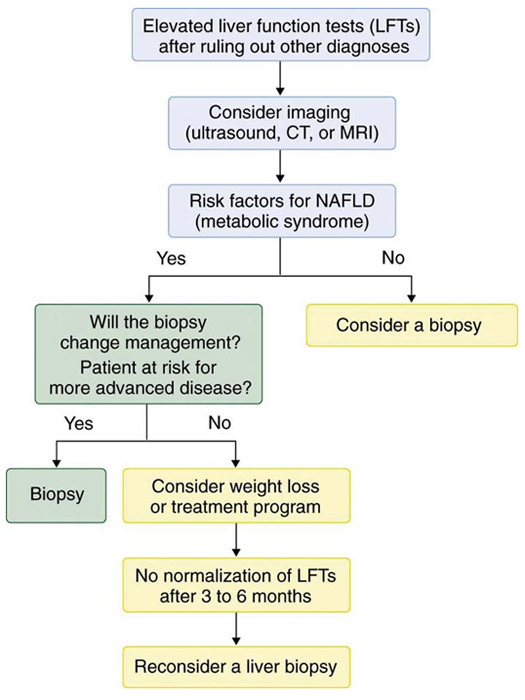
Despite the advantages of liver biopsy, its overall role in the evaluation of patients with NAFLD is unsettled, in large measure because of its risks and poor patient acceptance. In patients with risk factors for NAFLD (ie, metabolic syndrome), 3 to 6 months are often allowed for a trial of weight loss and for possible improvements in imaging studies and biochemical markers of liver disease. In the subset of patients most likely to have NASH or advanced disease (those older than 45 years, significant obesity, type 2 diabetes, multiple components of metabolic syndrome, low platelets, low albumin, AST/ALT ratio ≥1, evidence of portal hypertension) and in those with an unclear diagnosis, a liver biopsy should be considered earlier (Figure 3). A repeat liver biopsy in patients with NASH in 3-5 years should be considered to monitor disease progression.
Because of the important limitations of the currently available noninvasive and invasive tests, recent efforts have focused on identifying potential novel noninvasive biomarkers for NASH and assessment of fibrosis.
The goal of treatment is to improve steatosis and prevent the development of fibrosis, which can lead to cirrhosis and its complications. Because the prognosis of NASH depends on risk factors (eg, obesity, insulin resistance, type 2 diabetes), these conditions have been the focus of treatment. Treatment proposed for NAFLD has been based on the 2-insult hypothesis; the first being fatty liver infiltration (linked to obesity and insulin resistance) and the second being oxidative stress. Patients should avoid alcohol and other hepatotoxins.
Weight reduction has been widely studied in adults with NASH and has been shown to improve not only the biochemical results but also the histology. A review of 3 randomized controlled trials on weight reduction through lifestyle and pharmacologic intervention suggested that weight loss is safe and can improve histologic parameters of NASH. Slow, consistent weight loss through a diet designed to produce a caloric deficit of 500 to1000 kcal/day is advised. Reduction of dietary carbohydrates, in particular dietary fructose, is the most beneficial and has been found to improve the lipid profile in overweight patients. High- to moderate-intensity exercise (30 minutes, 3 to 5 times a week) has also been advocated to reduce the risk of comorbidities associated with obesity. However, more realistically, patients should be encouraged to incorporate moderate activity into everyday life (eg, climbing stairs, walking instead of driving).
Pharmacologic treatment of obesity in NASH is still experimental. Several drugs have been studied, including sibutramine, a serotonin reuptake inhibitor, and orlistat, which reduces fat absorption. Both of these have been shown to improve liver enzyme levels and sonographic signs of fatty liver. A meta-analysis of rimonabant, a cannabinoid-1-antagonist, showed that it is associated with increased adverse events and currently it cannot be recommended for NAFLD.
Finally, bariatric surgery is now suggested for patients with a BMI >40 kg/m2, or for those with a BMI of >35 kg/m2 and obesity-related comorbidities. Resolution in steatosis, but not of fibrosis, has been demonstrated. However, the safety of bariatric surgery in patients with cirrhosis is still under investigation. Randomized clinical trials are needed to determine if bariatric surgery is an appropriate therapy in NASH patients.
NASH patients with diabetes are at higher risk of developing more-aggressive disease. Insulin-sensitizing agents have been tested in adults. Metformin, a biguanide oral anti-diabetic agent, lowers hepatic glucose production and promotes glucose uptake in the muscles. Studies on metformin have shown discrepant results. Randomized controlled trials have shown improved serum liver enzymes and insulin resistance but inconsistent effects on liver histology. A large randomized trial in children with NASH did not show a sustained reduction in ALT or improvements in NAFLD activity score for histologic features in the liver.
Peroxisome proliferator-activated receptor gamma (PPARg) agonists (thioglitazones) have been shown to improve insulin resistance, a surrogate marker of fatty liver, and histology by promoting redistribution of triglycerides from the liver and muscle into proliferating adipocytes. Pioglitazone studies have shown conflicting results. A recent phase 3, randomized, placebo-controlled, double blind clinical trial on the use of pioglitazone versus vitamin E versus placebo for the treatment of non-diabetic patients with NASH (PIVENS trial) showed no difference in the rate of improvement in NASH compared with placebo but it did show a reduction in aminotransferases and hepatic steatosis. Longer term trials suggest that long term therapy with thioglitazones are needed to maintain histologic improvement but would offer no additional histologic benefit. Hepatotoxicity has been described with thioglitazones, and a more common side effect is paradoxical weight gain and fat redistribution. Although controversial, increased risk of cardiovascular events and bone loss with the use of rosiglitazone as well as of increased risk of heart failure with pioglitazone have been described.
The literature concerning lipid-lowering medication and NAFLD is sparse. Reports have demonstrated improvement in transaminase levels with different classes of drugs, but there is a lack of histologic follow-up. Fibrates, in one randomized controlled trial, did not show any histologic benefit. Probucol, a lipophilic lipid lowering drug, has shown improvement in aminotransferases but it can also reduce high density lipoprotein levels. Although one of the most common side effect of statins is liver enzyme level elevation, evidence has pointed out that patients with elevated baseline transaminase levels (likely having NAFLD) who receive statin treatment do not have a higher incidence of liver enzyme level elevation or hepatotoxicity than liver disease control subjects who do not receive statins. Moreover, the clinical relevance of the current recommendation that liver biochemistry should be checked before and periodically (usually 12 weeks) after treatment initiation has not been substantiated in the NAFLD population.
Oxidative stress has been hypothesized to contribute to the progression of NAFLD to NASH and to worsen insulin resistance. For this reason, antioxidant treatment to reduce this stress and slow the progression of the disease has been studied. Several small trials in humans with NAFLD have supported an effect of tocopherol (vitamin E) on the improvement of transaminase levels but there have been discordant results in histologic improvement. The recent larger PIVENS trial showed that vitamin E (800 IU/d) led to an improvement in NASH compared with placebo as well as a reduction in aminotransferases. However, a controversial report has shown a mild increase in all-cause mortality in people taking high-dose vitamin E (≥400 IU/d) as a health supplement.
Several therapeutic agents believed to offer hepatocyte protection have been evaluated. Despite small adult studies suggesting a role of ursodeoxycholic acid in the improvement of NASH, a large, randomized, placebo-controlled trial has demonstrated no benefits from ursodeoxycholic acid over placebo on liver biochemistry and histology. Pentoxifylline inhibits a number of proinflammatory cytokines and may have hepatoprotective effects. One small randomized study showed improvement in histologic features of NASH when compared with placebo. Betaine and N-acetylcysteine have shown promising effects, but larger trials are needed.
The renin-angiotensin system may induce fibrosis in NAFLD. Angiotensin-converting enzyme inhibitors and angiotensin-receptor blockers (ARBs) can improve insulin sensitivity. ARBs, in small studies including a randomized controlled trial, have shown improvement in histologic inflammation and fibrosis. Monounsaturated fatty acid intake improves cardiovascular risk and lipid profiles. Polyunsaturated fatty acids, studied in 3 randomized controlled trials, have been shown to improve biochemical and ultrasound features of liver steatosis (a phase II trial is underway).
In a randomized controlled trial, L-carnitine was found to improve steatosis, NAFLD histologic activity score and aminotransferases. Pilot studies based on the theory that NAFLD may be linked to small bowel bacterial overgrowth have shown some promise with the use of probiotics and prebiotics. An inverse association between coffee consumption and severity of fibrosis has been seen in multiple studies. Thus regular coffee consumption may be reasonable to recommend patients with NASH. Further advances in understanding the pathogenesis of NAFLD, such as induction of toll-like receptors leading to proinflammatory and profibrogenic cytokines which contribute to NASH, may also help to provide new therapeutic options for NASH.
Emerging data from recent trials have suggested that weight loss through lifestyle modifications, as well as several insulin-sensitizing, antioxidants, hepatoprotective medications and others, may be of benefit in patients with NAFLD (Table 3). In 2010, the Italian Association for the Study of the Liver and in 2012 the American Association for the Study of Liver Diseases in conjunction with the American College of Gastroenterology and the American Gastroenterological Association published evidence-based practice guidelines for the diagnosis and management of NAFLD. Both guidelines endorse lifestyle changes. A 3% to 4% loss in body weight likely improves steatosis, and weight of loss up to 10% may improve necro-inflammation. This can be achieved with a hypocaloric diet alone or in conjunction with exercise. Anti-obesity drugs are currently not recommended. Bariatric surgery in the appropriate individual may be useful to control obesity but the guidelines indicate that bariatric surgery is not yet an established option for the treatment of NASH.
Vitamin E is considered a first-line therapy in biopsy proven NASH in the practice guidelines although it is not advised in patients with diabetes or cirrhosis. Pioglitazone can be used to treat steatohepatitis in biopsy-proven NASH but long-term safety has not been established and it’s use in a NASH population with diabetes has not been studied. Metformin, ursodeoxycholic acid, and omega-3 fatty acids are not recommended. Statins are deemed safe to use to treat dyslipidemia but are not currently recommended to treat NASH specifically. Further studies are needed for other therapies before they can be formally recommended.
| Table 3. Therapeutic approaches for nonalcoholic fatty liver disease |
|---|
Weight Loss
|
Insulin-Sensitizing Agents
|
Lipid-Lowering Drugs
|
Antioxidants
|
Other Agents
|
* Practice Guideline Recommendation
Copyright © 2006 The Cleveland Clinic Foundation.
In patients with decompensated NAFLD cirrhosis, liver transplantation should be considered. Coexisting conditions (eg, morbid obesity, severe complications of diabetes, cardiac disease) and fear of intraoperative and post-transplantation complications, may preclude transplantation candidacy in these patients. A thorough pretransplantation evaluation, as well as better weight and metabolic derangement control, may be necessary. Following transplant, most patients have persistent metabolic syndrome, with long-term implications. Moreover, NAFLD has been shown to recur in the liver allograft, with a possible rapid progression to steatohepatitis and cirrhosis.
More than 50 million Americans have been estimated to have the metabolic syndrome, and 80% of them probably have NAFLD. Furthermore, about one-third of the US population suffering from type 2 diabetes mellitus has fatty liver. The prevalence of NAFLD in the US seems to be substantially greater than the 2% prevalence of hepatitis C virus infection and is believed to be increasing. Given such a high prevalence, the American Gastroenterological Association Technical Review on Nonalcoholic Fatty Liver Disease, published in 2002, stated that “physicians should actively check for the presence of NAFLD in those who are overweight and/or diabetic.” Screening is complicated by the fact that the accuracy of noninvasive diagnostic tools remains poor and, apart from weight loss, there is no clearly established treatment for NAFLD. Basic laboratory evaluation of liver enzyme levels might point to the diagnosis but cannot rule out NAFLD if test results are normal, and imaging techniques have poor sensitivity for low-grade steatosis. Moreover, because these tests do not differentiate simple steatosis from NASH, a liver biopsy must be discussed with the patient if the suspicion of NASH is strong. Therefore, although generalized screening for fatty liver in all at-risk patients may be difficult and is not recommended by the practice guidelines, it is certainly warranted to look for and actively manage the metabolic syndrome (obesity, diabetes, hyperlipidemia, and hypertension). Prevention of obesity and its complications is now a major public health goal.
NAFLD affects a substantial portion of the general population and is associated with metabolic syndrome, which includes obesity, insulin resistance, hyperlipidemia, and hypertension. Patients with NAFLD not only frequently suffer from insulin resistance but also have increased overall mortality. Although simple fatty liver seems to be a benign condition, it can progress to NASH and ultimately to cirrhosis in some patients. Because of the consequences of the disease, we emphasize the importance of the detection of NAFLD in high-risk groups, including obese patients, as well as those with evidence of insulin resistance or other components of metabolic syndrome. Screening and surveillance methods should be applied more uniformly from center to center, and reliable noninvasive techniques are needed to diagnose NAFLD and the detection of progressive liver disease. The diagnosis of NAFLD should prompt management of metabolic risk factors. Weight loss regimens are believed to be helpful, and numerous drugs have been investigated in small studies. Large randomized clinical trials are necessary to determine the real benefit of these agents. Finally, studies on the pathogenesis of NAFLD may not only improve our understanding of the mechanisms involved in NAFLD progression but also may lead to novel therapeutic strategies to treat this condition.