Published: July 2015
Vasculitis, referred to as angiitis, that affects the central nervous system (CNS) is one of the most formidable diagnostic and therapeutic challenges for physicians because the clinical manifestations of CNS vasculitis are highly variable, the CNS is a common target of many forms of systemic vasculitis and may also be the sole target of vasculitis, and specific noninvasive tests are lacking and material for pathophysiologic investigation is limited. Despite these challenges, we have witnessed a great progress in our understanding of the disease, and its subsets. Our ability to recognize and diagnose the mimics of CNS vasculitis have improved dramatically. Correct diagnosis still requires a high degree of suspicion coupled with knowledge of other diseases that can masquerade as vasculitis.
A primary vasculitis limited to the CNS is referred to as primary angiitis of the CNS (PACNS). A generalized systemic vasculitic process can also involve the CNS, and in such cases, it is referred to as secondary vasculitis of the CNS. Secondary vasculitis is not discussed in this chapter.
The earliest reports of PACNS described the disease as fatal and progressive, limited to the CNS, and characterized by rich granulomatous vasculitis. The disease was named granulomatous angiitis of the CNS (GACNS), and it remained a rare diagnostic entity until the 1980s. Increasing reports of successful treatment with cyclophosphamide and glucocorticoids as well as the use of angiography for the diagnosis of PACNS heightened the interest in the diagnosis. In 1988, Calabrese and Mallek1 proposed criteria for the diagnosis of PACNS (Box 1).
| Box 1: Proposed Criteria for Primary Angiitis of the Central Nervous System1 |
|---|
| The presence of an acquired and otherwise unexplained neurologic deficit |
| • With presence of either classic angiographic or histopathologic features of angiitis within the CNS |
| • And no evidence of systemic vasculitis or any condition that could elicit the angiographic or pathologic features |
Adapted from Calabrese LH, Mallek JA: Primary angiitis of the central nervous system: Report of 8 new cases, review of the literature, and proposal for diagnostic criteria. Medicine (Baltimore). 1988;67:20-39.
In the 1990s, we and others began to question whether PACNS is a homogeneous disease or whether different clinical subsets exist. A subset diagnosed on the basis of angiography and with a predictably more benign outcome requiring less–intensive therapy was identified and originally named benign angiopathy of the CNS (BACNS). Later on, it became clear that the pathophysiologic basis of BACNS is characterized by vasospasm and closely resembles other vasospastic disorders such as Call–Fleming syndrome, postpartum angiopathy, migrainous vasospasm, and drug–induced arteritis. The term reversible cerebral vasoconstriction syndromes (RCVS) have unified BACNS and other similar phenotypes under the same clinico–radiological syndromes.2 In our practice, RCVS represents a major mimic of PACNS and it will discussed in this chapter.
Over the years, it became clear that PACNS is not uniform but rather a heterogeneous disease with multiple presentations. Mass–like presentation occurs in 5% of the cases.3 The diagnosis is usually unexpected and is ascertained after pathologic findings of vasculitis in the excised mass. Other subsets include, spinal cord involvement in 5% of cases,4 leptomeningeal enhancement disease, and beta–related amyloid angiopathy, which is mostly seen in older patients.5
Primary angiitis of the CNS was first described in the mid–1950s. By 1986, only 46 cases had been reported in the English–language medical literature. Since 1975, an increasing number of cases have been described, and over 500 cases were reported through 2007. Primary angiitis of the CNS affects patients of all ages but peaks around 50 years of age and is most common in males. A retrospective analysis of 101 cases revealed that the average annual incidence of PACNS is 2.4 cases per 1 million person–years.6 Recently, CNS vasculitis was found to be one of the common misdiagnoses of patients with sporadic Creutzfeldt–Jakob disease, when a brain biopsy was used in the work up of dementia.7 Today, although PACNS is still uncommon, its specter is often raised in patients with neurologic problems of obscure origin, making its diagnostic approach a relevant clinical issue.
Primary angiitis of the CNS is a heterogeneous disease with different clinical subsets of unknown etiology and pathogenesis. The pathologically defined entity, GACNS, is primarily a leptomeningeal and cortical vasculitis involving the small and medium leptomeningeal and cortical arteries. Pathologic findings include classic granulomatous angiitis with Langhans' or foreign body giant cells, necrotizing vasculitis, or a lymphocytic vasculitis. The initial event that primes the inflammatory cells is not known. However, the final pathway of inflammation leads to occlusion of the involved blood vessel, thrombosis, and, ultimately, ischemia and necrosis of the territories of the involved vessels. Limited data suggest an association with systemic viral illnesses or a state of altered host defense and PACNS. Duna and colleagues8 analyzed 168 reported cases of PACNS and found that 29 of these were associated with an illness characterized by an immunosuppressive state, including corticosteroid therapy, lymphoproliferative or myeloproliferative disorders, and human immunodeficiency virus (HIV) infection. In addition, a variety of pathogens have been documented in association with CNS arteritis, including varicella zoster virus (VZV), HIV, and cytomegalovirus.9–11
It is likely that in the setting of altered host defense mechanisms or in a predisposed patient, a pathogen escapes immune defense mechanisms and induces arteritis. In support of this hypothesis is the well–defined clinical syndrome of post–herpes zoster ophthalmicus contralateral hemiplegia. In this syndrome, a contralateral hemiplegia occurs weeks to months after VZV infection of the trigeminal ganglion and nerve, apparently resulting from the retrograde spread of VZV to intracranial vessels. Viral particles have been identified in the cytoplasm and nuclei of smooth muscle cells within the walls of affected vessels. Human immunodeficiency virus infection has been similarly described in such a setting.10,12
The clinical signs and symptoms of PACNS are nonspecific and reflect the diffuse and often patchy nature of the pathological process. The course of the illness is also variable with presentations ranging from hyperacute to chronic and insidious. In patients with the disease variant GACNS, characterized by a presentation of chronic meningitis and a small–vessel distribution, signs or symptoms might precede diagnosis by 3 years or more.6,13
The most common symptoms of PACNS are headaches, followed by neurologic deficits. The headache varies in description, intensity, and pattern. It is usually chronic and insidious. We believe that thunderclap headaches are not a feature of PACNS and their presence should indicate a diagnosis of RCVS.2 Other symptoms include cognitive impairment, stroke, and transient ischaemic attacks occurring in 30% to 50% of patients with PACNS (Box 2).6,13 Strokes are usually multiple and vary in age. Cranial nerve can be rarely affected, in addition to myelopathy, seizures, and ataxia.
| Box 2: Clinical Features of Primary Angiitis of the Central Nervous System |
|---|
|
It is important to note that signs and symptoms of systemic inflammatory process including marked constitutional symptoms, weight loss, or visceral target–organ disease are not typical of PACNS and should raise the likelihood of systemic illnesses.
The most common scenarios where PACNS is considered include: (a) multiple cerebral ischemia, affecting different vascular territories in association with inflammatory pattern in the cerebrospinal fluid (CSF); (b) subacute or chronic headache with cognitive impairment or chronic aseptic meningitis; and (c) chronic meningitis presentation after infectious and neoplastic disorders have been ruled out.
Reversible cerebral vasoconstrictive syndrome is characterized by a set of clinical findings and diffuse spasms on cerebrovascular studies. In rheumatology, the term, benign angiopathy of the CNS, was initially proposed in 1993 to define case reports and clinical series of cases diagnosed on the basis of angiography alone that had far more benign outcomes than those described for PACNS. This nomenclature has evolved further into RCVS.14 Currently, RCVS is well accepted in the literature as a clinicoradiological syndrome characterized by recurrent thunderclap headache with or without neurologic symptoms in addition to reversible vasoconstriction of cerebral arteries. It affects patients of various ethnic groups and in all age groups but most commonly in the fourth decade of life. Many conditions and exposures have been linked to RCVS including vasoactive drugs and the peripartum period. Disturbance of the cerebral vascular tone is thought to contribute to the disease's pathophysiology. Reversible cerebral vasoconstrictive syndrome generally follows a monophasic course. Associated strokes and cerebral hemorrhages occur in around one–third of the patients.
Recurrent thunderclap headache is the hallmark of RCVS occurring in more than 95% of patients; presentation is usually dramatic with the "worst ever" headache; this reaches its peak intensity in less than a minute. Although a single attack is possible, attacks typically recur over a 1 to 4 week period with an average of 4 attacks throughout the presentation. About 50% of patients report a residual mild intensity headache in between the severe exacerbations. Interestingly, patients usually are able to identify a trigger for the exacerbations such as strenuous exercise, sexual activity, bathing, swimming, coughing, sneezing, defecating, urinating, laughing, or other valsalva triggering maneuvers.
Reversible cerebral vasoconstrictive syndrome has been associated with different exposures with 30% to 60% of the cases. The most notable associations are vasoactive medications, pregnancy complications, and the puerperium. Various vasoactive medications have as well been incriminated including selective serotonin reuptake inhibitors, alpha–sympathomimetics of decongestants, hydroxycut and other diet pills, and acute migraine medications. Most illicit drugs have as well been implicated including cocaine and cannabis.15,16
Focal neurologic deficits and seizures can be a manifestation of RCVS. Neurologic symptoms and seizures vary between 8% to 43% and 1% and 17% of cases, respectively. Other symptoms including hemiplegia, dysarthria, aphasia, numbness, or ataxia can also occur. Most deficits are usually transient and resolve within minutes to a few hours. Persistent deficits would suggest a stroke (ischemic or hemorrhagic). Ischemic infarctions can occur in up to 39% of the cases. Infarctions can be multiple, bilateral, and symmetric and tend to occur in arterial brain watershed areas; cortical subarachnoid hemorrhages (SAH) occurs in a third of cases cohorts and are limited to few sulci near the convexity unilaterally or bilaterally. Intracerebral hemorrhages occur in 12% to 20% of patients and tend to be single, lobar, and concomitant with other lesions. Posterior reversible encephalopathy syndrome shares many clinical features with RCVS including headache, seizures, and visual disturbance and has been reported to occur in 10% to 38% of RCVS cases. Noteworthy is that despite the reversible nature of the cerebral vasoconstriction, given the prolonged nature of the process, permanent damage could ensue in around 10% of patients. Moreover, in less than 5% of patients, progressive vasoconstriction occurs resulting in major ischemic and hemorrhagic strokes, progressive brain edema, and potentially death.
Calabrese at al.2 proposed the first diagnostic criteria for RCVS emphasizing 5 points that must be fulfilled for a diagnosis of definative RCVS to be made (Table 1).
| Acute severe headache, often thunderclap with or without neurologic signs and symptoms |
| Demonstration of multifocal segmental cerebral artery vasoconstriction via direct (catheter) or indirect angiography |
| Absence of aneurysmal subarachnoid hemorrhage |
| Normal, or near normal, cerebrospinal fluid analysis |
| Demonstration of reversibility of angiographic finings within 12 weeks of disease onset |
Initial evaluation should be focused on excluding other diagnoses such as aneurysmal SAH, sentinel bleed, parenchymal hemorrhage, ischemic stroke, pituitary apoplexy, cerebral artery dissection, cerebral venous sinus thrombosis, meningitis, spontaneous intracranial hypotension, and cerebral vasculitis. An unenhanced brain computed tomography (CT) is uniformly the first–line imaging modality to exclude a subarachnoid or a parenchymal hemorrhage. Cerebrospinal fluid analysis is helpful in excluding inflammation as is seen in vasculitis or an infectious process. Normal CSF analysis is expected in RCVS with minor abnormalities occurring in the context of cortical SAH If indeed the CSF analysis is benign, then further brain and cerebrovascular imaging should include magnetic resonance imaging (MRI), MR angiography, and MR venography to further exclude alternate etiologies.
The diagnosis of RCVS rests upon the demonstration of diffuse reversible cerebral vasoconstriction. Cerebral vascular evaluation is thus warranted; while the gold standard remains catheter angiography, the sensitivity of indirect angiographic imaging (MR or CT angiography) is about 70%. These modalities demonstrate the characteristic diffuse "string of beads" appearance of the cerebral arteries indicating segmental narrowing and dilatation. Affected vessels usually are bilateral, diffuse, and include the anterior and posterior circulation. It is very important to realize the dynamic nature of the disease process as the vasoconstriction is not fixed; thus a repeat angiography in a few days would show resolution at some vessels with potentially new constrictions.
It should be emphasized that while cerebral angiogranphic findings are suggestive of RCVS, they are in no way specific. Cerebral segmental narrowing and dilatation can also be seen in atherosclerosis, infectious arteritis, inflammatory vasculitis, and fibromuscular dysplasia. The most specific evidence for RCVS is the demonstration of resolution of vasoconstriction within a 12–week period.
Reversible cerebral vasoconstrictive syndrome follows a monophasic course with complete resolution of all signs and symptoms in the vast majority patients. In the right clinical setting, diagnosis rests upon ruling out other potential etiologies and demonstrating reversible cerebral vasoconstriction via repeated cerebrovascular studies. Watchful waiting is a reasonable management plan given the self–limiting nature of the disease with focus on symptom control and precipitant avoidance.
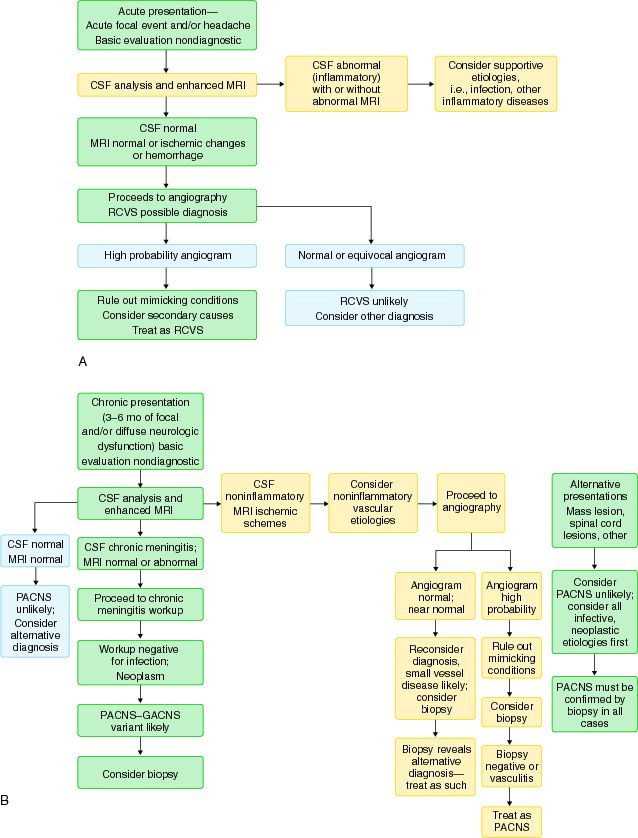
The approach to patients with suspected PACNS is not uniform and varies depending on the clinical presentations. In most instances, and depending on the clinical setting, the diagnosis of CNS vasculitis is secured by either a positive biopsy or high–probability vascular imaging, such as angiography, while excluding other conditions that can mimic the disease (Figure 1). Important conditions that can manifest as PACNS and that should be excluded before making any definitive diagnosis include infections, neoplasms, drug exposure, vasospastic disorders, systemic vasculitides, and vasculopathies (Box 3). In our clinical practice, RCVS represent the most common mimics of PACNS.
| Box 3: Mimics of Primary Angiitis of the Central Nervous System |
|---|
Systemic Vasculitides and Connective Tissue Diseases
|
Infection
|
Neoplasm
|
Miscellaneous
|
No blood studies are diagnostic for CNS vasculitis. Acute–phase reactants, such as sedimentation rate and C–reactive protein, are usually normal in patients with PACNS. If serum markers of inflammation are elevated, secondary forms of CNS vasculitis should be evaluated. If the history and physical examination point to a systemic vasculitis, testing should proceed accordingly. Testing for a variety of infectious organisms, such as mycobacteria, fungi, and HIV, is warranted in patients presenting with chronic meningitis. Other serologic tests are indicated if there is a history of exposure, such as tick bites in Lyme disease. Evaluation for hypercoagulable states and emboli and investigation of drug exposure, including over–the–counter medications, are essential in patients who present with acute focal or multifocal disease.
Analysis of the CSF is essential. It is an essential diagnostic tool in patients with suspected CNS vasculitis and is of great value in ruling out infectious mimics. Cerebrospinal fluid findings are abnormal in 80% to 90% of pathologically documented cases of PACNS. Findings usually reflect aseptic meningitis, with modest pleocytosis and elevated protein levels with a negative infectious workup. The importance of obtaining appropriate stains, cultures, and serology evaluations to exclude any infectious etiologies cannot be overstressed, especially in patients presenting with chronic meningitis. In contract to PACNS, patients with RCVS typically have a normal or near–normal CSF analysis.
Neuroimaging studies, such as CT and MRI, are important in the diagnosis of PACNS but are not specific or sufficient for diagnosis. Magnetic resonance imaging is a more sensitive diagnostic imaging technique than CT in CNS vasculitis, and it should be the initial study of choice when approaching a patient with unexplained ischemia, except when cerebral hemorrhage is suspected. Magnetic resonance imaging is very sensitive in detecting abnormalities in PACNS. The sensitivity of MRI in PACNS has been reported as low as 75% or approaching 100%.17 Interpretation of figures derived from older series is limited since because most series were confounded by inclusion of many patients with RCVS. Findings on MRI are variable and include multiple and often bilateral infarcts in cortex, deep white matter, or leptomeninges, with or without contrast enhancement. Sites of contrast enhancement in the leptomeninges provide ideal places for biopsy and can increase the yield for a positive biopsy. Advanced neuroradiographic techniques such as the inclusion of diffusion– and fluid–attenuated inversion recovery MRI sequences, single photon emission CT, or positron emission tomography increase the sensitivity of finding abnormalities but not the specificity for diagnosis. Combining neuroimaging with lumbar puncture increases the overall sensitivity; a normal MRI along with normal CSF have a high negative predictive value against a diagnosis of PACNS. Progresses in radiologic modalities include high– resolution multicontrast wall and lumen MRI, which is an encouraging modality in PACNS. The advantage of this technique is in its ability to provide details of not only the lumen of the affected vessels but, more interestingly, details about the wall structure of the intracranial blood vessels. This modality may enhance the test specificity in CNS vasculopathies.18
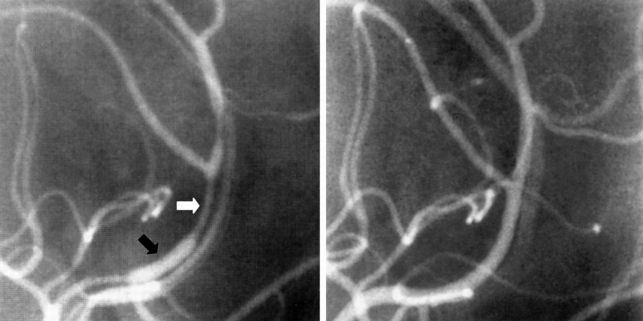
Angiography is a vital diagnostic modality in evaluating patients with CNS vasculitis provided that its limited specificity and lack of quantitative and qualitative codification are appreciated. Cerebral angiography is limited by several factors. Its sensitivity decreases with the caliber of the vessel, being most sensitive for disease of larger vessels. In pathologically proven cases, such as GACNS where the pathologic involvement is predominantly in the small penetrating vessels beneath the leptomeninges, cerebral angiography findings are generally normal.19 Moreover, the interpretation of the angiographic findings is often limited by poor specificity (26%).20 Findings on angiography include alteration of the vessel caliber (ie, beading) and absence or cutoff of 1 or more vessels (see Figure 2). These types of changes may be seen in multiple vessels in multiple vascular beds or may be limited to a single vessel. These findings are not diagnostic and can be encountered in vasospastic, infectious, embolic, and atherosclerotic diseases and in hypercoagulable states and they should be carefully interpreted. In patients with RCVS, involvement of multiple vessels in multiple vascular beds (high–probability angiogram) is characteristic, and documentation of reversibility of the angiographic abnormalities, along the course of the disease, is essential to secure the diagnosis (see Figure 3.)
Histologic confirmation of vasculitis is considered the standard for the diagnosis of CNS vasculitis, but brain biopsy is also limited by several factors. First, the procedure is highly invasive and requires the skills of an experienced neurosurgeon, who might not always be available. Second, the technical aspects of the procedures should be tailored to the individual patient. In patients with suspected GACNS, the procedure of choice is open–wedge biopsy of the tip of the non–dominant temporal lobe with sampling of the overlying leptomeninges and underlying cortex. Alternatively, directing the biopsy to an area of leptomeningeal enhancement, when present, might increase the sensitivity.21 Central nervous system vasculitis is a notoriously patchy disease, which limits the sensitivity of the procedure, and as many as 25% of the biopsies are falsely negative.19 Finally, the presence of vasculitis in the biopsy specimen should not preclude performing special stains and cultures for occult infections or malignancies that can produce secondary vascular inflammation.
Multiple disorders are capable of mimicking the clinical and angiographic picture of CNS vasculitis, while others conditions are associated with true CNS vasculitis. It is prudent to exclude mimics of the disease before securing the diagnosis of PACNS.9, 22 Cerebral arteriopathies that can mimic PACNS include atherosclerosis small–vessel disease due to diabetes, dyslipedaemia, and hypertension, Moyamoya disease, intracranial artery dissection, and arteriopathy secondary to remote cranial irradiation.22 Other entities such as embolic and hypercoagulable disorders should be excluded. The presence of retinal disease and or inner ear disease suggestive of cochlear dysfunction should raise the spectrum of retinocochleocerebral vasculopathy and in particular Susac's syndrome. Lastly, a family history of unexplained CNS disease should prompt a search for a number of genetic variants, including cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL), its autosomal recessive variant (CARASIL), retinal vasculopathy with cerebral leukodystrophy (RVCL), and others.17
Central nervous system vasculitis can occur in the setting of different systemic inflammatory/infectious diseases such as systemic vasculitides, connective tissue disease, sarcoidosis or infections. Infectious–related CNS vasculitides are crucial to exclude and are discussed in a different chapter. Central nervous system disease in the setting of systemic inflammatory conditions poses multiple challenges. Before attributing the CNS disease to the systemic process, infections and metabolic etiologies should be ruled out especially in patients who are immunocompromised. Most common systemic vasculitides with secondary CNS involvement include Behcet's syndrome, granulomatosis with polyangiitis (Wegener), polyarteritis nodosa (PAN), microscopic polyangiitis (MPA), and eosinophilic granulomatosis with polyangiitis (Churg–Strauss syndrome).17 Central nervous system involvement is not uncommon in connective tissue diseases, mainly systemic lupus erythematosus (SLE) and Sjogren's syndrome.17 However the vasculopathy in SLE is characterized by small– vessel hyalinization, thickening, intramural platelet deposition, and thrombus formation. Frank CNS vasculitis occurs in less than 7% of cases of SLE.17 One of the most frequently encountered mimics in our practice is RCVS.
It is crucial to differentiate between RCVS and PACNS (Table 2). There is overlap between the 2 entities on multiple levels and misdiagnosis is common. Common clinical features of both RCVS and PACNS include headaches, seizures, strokes, and abnormal cerebrovascular imaging. However the headaches in RCVS are thunderclap in nature in contrast to insidious and the chronic headaches encountered in PACNS. History of vasoconstrictive drug exposure or recent childbirth, are associated in RCVS. The CSF is normal or near normal in RCVS in contrast to abnormal values seen in PACNS. At the radiological level PACNS is rarely associated with normal brain parenchymal imaging or haemorrhagic lesions. In contrast, patients with RCVS can have severe vasoconstriction without parenchymal lesions; lobar and cortical surface subarachnoid haemorrhages, as well as reversible edematous lesions similar to the lesions of the posterior reversible leukoencephalopathy syndrome, are common. Finally, in RCVS, the angiographic abnormalities are dynamic, more severe, and typically resolve over a period of weeks to 3 months. Nevertheless, in some cases differentiating PACNS from RCVS remains challenging, giving the false–negative brain biopsy in PACNS and the absence of confirmatory serological tests for PACNS. Ongoing research using high–resolution MRI shows promise in distinguishing the various causes of cerebral arteriopathies based on the presence and the pattern (eg, concentric vs. eccentric) of vessel wall contrast enhancement.23
| RCVS | PACNS | |
|---|---|---|
| Patients | Female–predominant | Male–predominant |
| Disease onset | Acute | Chronic |
| Clinical course | Monophasic | Chronic |
| CSF findings | Normal | Abnormal |
| Abnormal angiography | 100% | 50% |
| Treatment | CCB | GC and CYC |
| Outcomes | Excellent | Good |
CCB = calcium channel blockers; CSF = cerebrospinal fluid; CYC = cyclophosphamide; GC = glucocorticoids; PACNS = primary angiitis of the central nervous system; RCVS = reversible cerebral vasoconstriction syndrome.
Several issues emerge when treating CNS vasculitis. An accurate diagnosis, the most important initial step, is hampered by the protean manifestations of the disease and the lack of specific and sensitive noninvasive studies coupled with the low specificity and test efficiency of the invasive studies, such as biopsy and angiography. At the same time, diagnosis and treatment are urgent to avoid permanent neurologic damage. A major problem for clinicians is how to monitor disease activity and not confuse irreversible target–organ damage with treatment–resistant disease.
There are no controlled studies of therapy for PACNS, and therapeutic guidelines are based largely on experts' consensus opinion. On the basis of the historical literature, cases with granulomatous pathologic findings carry a progressive and highly lethal course; thus, patients are treated with a combination regimen of cyclophosphamide and glucocorticoids. Originally, cyclophosphamide treatment was continued for approximately 1 year after remission. More recently, and similar to the treatment of small vessel vasculitides, the goal is to limit exposure to alkylating agents by treating with oral cyclophosphamide for 3 to 6 months and, once the patient is in remission, to switch to an antimetabolite such as azathioprine or mycophenolate mofetil for maintenance therapy. Oral glucocorticoids are used, starting with a dose of 1 mg/kg/day of oral prednisone and gradually tapering to a small daily dose over 8 to 12 weeks. Initially, high dose pulse steroid may be required. For cases with a less disease burden, glucocorticoids alone may be sufficient. Assessment of disease activity includes monitoring of any new neurologic event, and serial MRI examinations. Serial MRI examinations are performed primarily to search for silent progression during tapering of therapy rather than to look for radiographic resolution. Adjunctive therapies, such as prophylaxis for Pneumocystis jirovecii infection and adequate prophylaxis for osteoporosis, should be implemented to avoid treatment–related toxicities.
Earlier descriptions characterized PACNS as a fatal disease, and most cases were diagnosed postmortem. In the early 1980s, reports of successful treatment emerged and physicians became more interested in the diagnosis of CNS vasculitis. With better understanding of the subsets of the disease, the advancing therapy, and treatment–related toxicities as well as the advent of neuroradiology, more favorable outcomes and improving mortality rate have been reported.
We have studied the long–term outcomes of 54 patients with PACNS at Cleveland Clinic. Forty–one patients with PACNS were interviewed and their outcomes were analyzed using the Barthel Index, a validated scale used for patients with stroke, as well as a new scale developed expressly for this investigation (cognitive index).24 Overall, the outcome was favorable, with a 29% (16 of 54 patients) relapse rate and 10% mortality rate (5 of 54 patients). Eighty percent (33 of 41 patients) of the interviewed patients demonstrated mild to no impairment on the Barthel Index. Using the cognitive index, mild deficits of concentration and memory and decreased energy level were the most common symptoms.24