Published: September 2018
Expire: September 2021
More than 5 million cases of skin cancer will be diagnosed in the United States this year. Although nonmelanoma skin cancer such as basal cell carcinoma and squamous cell carcinoma is the most common type of malignancy in humans, melanoma ranks as the sixth most common cancer in the United States and accounts for 1 death per hour. It has been estimated that 86% of melanomas can be attributed to exposure to ultraviolet (UV) radiation. A person’s risk of melanoma doubles after 5 sunburns; it is halved with regular use of a sunscreen with a sun protection factor (SPF) of 15 or higher.1
The incidence rate of nonmelanoma skin cancer is staggering, having increased by 77% between 1994 and 2014; however, the cure rate is better than 95% if detected and treated early. The incidence of melanoma is also skyrocketing, and the mortality rate is higher with melanoma. Cure rates for localized primary cutaneous melanoma are excellent if caught early and treated appropriately. Within the previous 10 years, a number of advances have been made in the treatment of melanoma metastatic to lymph nodes and distant organs, including the use of targeted therapies and immunotherapies. Early detection has led to overall increased survival rates for melanoma patients. Thus, it is of utmost importance for all physicians to possess the clinical diagnostic skills necessary to identify melanoma and refer patients for evaluation and treatment.2
Primary cutaneous melanoma is a malignant neoplasm arising from melanocytes, the skin’s pigment-producing cells; it can occur de novo or within a preexisting lesion such as a congenital, acquired, or atypical (dysplastic) nevus. Noncutaneous primary sites of melanocytes also include the mucosal epithelium, retina, and leptomeninges. Cure is much more likely after surgical excision when a lesion is detected early in its development.3 Prompt detection, diagnosis, and adequate removal of the lesion are of utmost importance, as a delay of even 30 days increases the risk of death.4
Education of the public with regard to the technique of routine self-examination and proper methods of sun protection can greatly improve the chances for early detection and adequate treatment of melanoma Box 1. A multidisciplinary approach, including primary care physicians, dermatologists, surgeons, oncologists, radiation oncologists, immunologists, radiologists, pathologists, and epidemiologists, is necessary to optimize detection and treatment of this increasingly common cancer.4
| Box 1: American Academy of Dermatology Sun Safety Tips |
|---|
| Because exposure to ultraviolet light contributes to the formation of skin cancer, dermatologists recommend the following precautions: |
| Avoid peak sunlight hours—10 a.m. until 4 p.m.—when the sun's rays are the strongest. |
| Apply a broad-spectrum sunscreen with a sun protection factor (SPF) of 15 or higher. Sunscreens may only be labeled “broad spectrum” if they include one or a combination of ingredients that protect against ultraviolet A and ultraviolet B radiation. |
| Reapply sunscreen every 1.5-2 hours, especially after swimming or heavy perspiration. |
| Wear sun-protective clothing including a wide-brimmed hat, sunglasses, long-sleeved shirt, and long pants. |
| Apply lip balm that contains sunscreen with an SPF 15 or higher. |
| Seek shade while outdoors during the day. |
| Protect children by minimizing sun exposure and by regularly applying sunscreen after the age of 6 months. |
| Be aware that surfaces such as water, snow, and sand can reflect up to 85% of the sun's damaging rays. |
| Avoid tanning beds. |
Adapted from Sober AJ, Chuang TY, Duvic M, et al; Guidelines/Outcomes Committee. Guidelines of care for primary cutaneous melanoma. J Am Acad Dermatol 2001; 45:579-586. © 2002 The Cleveland Clinic Foundation.
The incidence of melanoma is increasing across all ages, including a more than 600% increase in young adults from 1970 to 2009 [5]. Melanoma is the sixth most common cancer in men and women and the second most common cancer in women ages 20 to 29 in the United States.
Based on the most recent US data, there will be about 178,560 new cases of melanoma in 2018: 87,290 in situ (noninvasive) and 91,270 invasive. At current rates, 1 in 27 white men and 1 in 42 white women will develop an invasive melanoma over a lifetime. An estimated 9,320 people will die of melanoma in 2018: 5,990 men and 3,330 women. Apart from these statistics, if melanoma is detected and treated before it invades the deeper layers of skin, the 5-year survival rate is 99%. 2,3
The primary risk factor for melanoma is exposure to UV radiation [1]. Most melanomas arise in previously normal skin, and only 20% to 30% arise from pre-existing nevi. Although there are several genetic syndromes that predispose individuals to melanoma, these account for less than 15% of melanomas. These syndromes include xeroderma pigmentosa and familial atypical mole-melanoma syndrome (also known as dysplastic nevus syndrome).2,3
Evidence from epidemiologic studies shows that exposure to solar irradiation is the main cause of cutaneous melanoma in people prone to sunburn.6,7 This causal relationship is supported by anatomic site differences by sex, migration studies, latitude of residence, and race.
The most common site for melanoma in men is the upper back; in women, the most common sites are the lower legs and upper back.6 Studies have also shown that persons who immigrated to countries with higher levels of ambient solar radiation have higher rates of melanoma than similar people who did not move. Likewise, melanoma incidence and mortality rates in whites were inversely correlated with distance from the equator. Racial differences also exist with respect to melanoma. The lower rate of melanoma in darkly pigmented people results from the protective effect of melanin and the smaller number of nevi that can serve as precursor lesions for melanoma.
The main risk factors for cutaneous melanoma include phenotype (blue eyes, blond or red hair, fair complexion), cutaneous reaction to sun exposure (freckling, inability to tan, sunburn tendency), history of severe (blistering) sunburn or intense intermittent sun exposure, upper socioeconomic status, family history of melanoma, number and subtypes of nevi (atypical nevi or giant melanocytic nevi), history of melanoma, and immunosuppression.6,8
Genetic studies have also shown that 50% of familial melanomas and 25% of sporadic melanomas may be due to mutations in the tumor suppressor protein p16. Linkage studies have identified chromosome 9p21 as the familial melanoma gene.9 From 8% to 12% of all melanomas are familial melanoma. Familial atypical mole-melanoma syndrome has been defined as melanoma in 1 or more first- or second-degree relatives, as large numbers of melanocytic nevi (often 50 to 100 or more), some of which are atypical and varied in size, and as melanocytic nevi demonstrating certain histologic features. The mode of inheritance is most likely polygenic. The cumulative risk of developing cutaneous melanoma in persons with a history of familial melanoma is estimated to be 50% by age 50.9
Mutations in the gene CDKN2A within the 9p21 region have been demonstrated in familial melanoma kindreds. The CDKN2A gene is complex and codes for the p16 and p14arf proteins, both of which function to suppress cellular growth. Intact p16 inhibits cyclin-dependent kinases, a critical class of enzymes whose function is to promote cellular proliferation by inhibiting the retinoblastoma protein. Therefore, intact p16 is essential to arrest the cell cycle. The p14(ARF) protein may be important in enhancing the effect of another tumor suppressor, p53.9
The MAPK and PI3K-AKT molecular signaling pathways that allow for cell proliferation and survival are of critical importance in many melanomas; discovery of several abnormal proteins in this pathway responsible tumorigenesis has allowed for the development of targeted therapies in this pathway (see below). Among sporadic melanomas, almost half have mutations in the BRAF gene, including a common point mutation encoding for an altered protein, BRAFV600E. The MEK gene product is one step down the pathway from BRAF and can become altered in tumors that are “resistant” to targeted BRAF inhibitors.
Mutations in c-KIT, a receptor tyrosine kinase involved in initiating the pathway, are rare overall but can be seen in certain types of melanoma: acral melanoma, mucosal melanoma, and melanoma arising in areas of intermittent, intense sun exposure. Activating mutations at any point in the MAPK and PI3K-AKT pathways result in increased cellular proliferation and survival advantages of tumor cells.10
Because melanoma is the result of malignant degeneration of pigment-producing skin cells, most signs are related to a localized disordered production of pigment. Early signs of melanoma include the “ABCDE” criteria: asymmetry of the lesion; border irregularity, bleeding, or crusting; color change or variegation (some lesions are amelanotic [nonpigmented]); diameter larger than 6 mm, or growing; evolving (surface changes [raised, bleeding, crusting] or symptomatic [itchiness or tenderness]). The clinical differential diagnosis is listed in Box 2.1-3
| Box 2: Clinical Differential Diagnosis of Melanoma |
|---|
| Benign melanocytic lesion, such as nevus or solar lentigo |
| Atypical nevus |
| Squamous cell carcinoma |
| Pigmented basal cell carcinoma |
| Pyogenic granuloma |
| Seborrheic keratosis |
About 1% to 2% of primary melanomas arise from mucous membrane melanocytes. From 5% to 10% of patients present with metastatic disease (usually in the lymph node basin) without an identifiable primary lesion. Less than 2% of patients present with visceral metastases in the absence of an unknown primary lesion.11
Acquired atypical nevi (Figure 1) are melanocytic tumors that meet 1 or more of the ABCDE criteria and are characterized histologically by intraepidermal melanocytic dysplasia. The degree of melanocyte dysplasia is generally graded on a spectrum, with most dermatopathologists using a mild-moderate-severe scale based on the size and morphology of the dysplastic cells. Atypical nevi are important because they are potential precursors of melanoma and markers of increased melanoma risk. Atypical nevi are fairly common: 1.8% to 4.9% of white US adults have atypical nevi. Atypical nevi often start as rather large moles during the first decade of life.12 In a study of melanoma-prone families, almost 40% of children had dysplastic nevi, and all children in whom melanoma eventually developed had dysplastic nevi;13 children with dysplastic nevi and a family history of melanoma should be considered at high risk for melanoma. At least 17% of white adults with melanoma outside the familial melanoma setting have one or more atypical nevi, illustrating that atypical nevi are markers of risk.
Clinically, atypical nevi appear by age 20 as pink or brown macules or papules with 2 or more disorderly distributed shades of brown and black. They may be round, oval, or misshapen, with an irregular or fuzzy outline. Any site may be affected, even sites not exposed to the sun. The “horse-collar” area (ie, chest, shoulders, and upper back) are usually most heavily involved.14
Atypical nevi can remain unchanged, progress to melanoma, or regress over time. Only a small fraction progress to melanoma, even in patients with a family history of melanoma, and environmental, genetic, and immunologic factors likely play a role in the transition to melanoma. In a different study of melanoma-prone families, persons with atypical nevi had a 56% chance of developing melanoma between ages 20 and 59.14
Atypical nevi should be considered potential precursors of melanoma and thus deserve careful surveillance and prompt treatment when required. However, the optimal management of atypical nevi remains controversial for patients with or without a personal or family history of melanoma. For people who have 1 or 2 clinically atypical nevi, prophylactic excision is reasonable, but regular skin self-examination and periodic in-office examinations should be recommended for life.12 Prophylactic removal of large numbers of atypical nevi is neither feasible nor desirable; however, excision for hard-to-monitor areas (eg, scalp, perineum) should be considered, and serial clinical photography of other lesions should be performed to detect new or changing nevi. Persons with atypical nevi should also be instructed on how to practice skin self-examination every 4 to 6 weeks at home.12,16
Pathologic confirmation of the clinical diagnosis provides a basis for making further management decisions. Generally, atypical nevi with mild and moderate melanocytic dysplasia can be monitored clinically after biopsy without follow-up excision. If an atypical nevus recurs after shave biopsy, the scar associated with the initial procedure can make pathologic diagnosis challenging, and the history of the lesion should be presented to the interpreting dermatopathologist. Rather than using shave biopsy, some authors advocate an initial diagnostic and therapeutic procedure with punch biopsy with a 1- to 2-mm margin around the clinically apparent nevus, to reduce the risk of recurrence. However, this approach should be discussed with the patient, given the more invasive nature of the procedure with increased scar formation.15,16
For the removal of atypical nevi with severe melanocytic dysplasia, lateral margins of 3 to 5 mm should be taken to ensure complete removal.12
A short discussion on congenital nevi (Figure 2) is presented here because patients are often concerned about the malignant potential of these lesions.17 A congenital nevus is defined as a melanocytic nevus that is present at birth or appears within the first few months of life. They are classified by size as small (< 1.5 cm), medium (1.5-20 cm), and large (> 20.0 cm). The risk of cutaneous melanoma developing within small- and medium-sized lesions is low, up to 1% over a lifetime, whereas the risk is up to 10% over a lifetime for large congenital nevi. Approximately 50% of melanomas that develop within large congenital nevi do so by age 3 to 5, and the melanoma risk is 5% during the first 5 years of life.9 Therefore, smaller congenital nevi can be followed clinically, but early and complete surgical excision of large congenital nevi is usually recommended. If complete removal is not possible, the lesion should be closely observed and any nodules or suspicious changes should be biopsied.12
Subtypes of melanoma are distinguished by clinical and pathologic growth patterns: lentigo maligna, superficial spreading, nodular, and acral lentiginous.
Lentigo maligna, a subtype of melanoma in situ (Figure 3), begins as an irregular tan macule that spreads peripherally, developing multiple shades of tan and brown throughout. It occurs on sun-damaged skin in elderly fair-skinned persons. Lentigo maligna is rapidly increasing in incidence, and represents the most common form of melanoma in certain geographic areas. The lesion can grow slowly for 5 to 15 years in the in situ form before becoming invasive.18 The exact percentage of lentigo maligna lesions that progress to invasive lentigo maligna melanoma is unknown but is estimated to be less than 30% to 50%. Although lentigo maligna has a prolonged radial growth phase, when invasion occurs, the result can be lethal. Long-term cumulative rather than intermittent sun exposure is believed to confer the greatest risk for developing lentigo malign.19
Although lentigo maligna is becoming more common, lentigo maligna melanoma remains a relatively uncommon subtype of melanoma, accounting for 4% to 15% of all melanoma patients. Lentigo maligna melanoma occurs almost exclusively on sun-exposed skin of the head and neck; the nose and cheeks are the most common sites. The median age at diagnosis is 65. The lesion is usually quite large (3-6 cm or larger), with a nodular area from 1 mm to 2 cm in width. Rarely, lentigo maligna and lentigo maligna melanoma are amelanotic, appearing as a pink patch or papule.20
Superficial spreading melanoma (Figure 4) is the most common type of melanoma, representing 70% of all melanomas, and is the most common type of cutaneous melanoma occurring in light-skinned people and in young people. It affects adults of all ages, with the peak incidence in the fourth and fifth decades of life. It most commonly affects intermittently sun-exposed areas with the greatest nevus density, such as the upper back of men and women and lower legs of women.
It is first noted as a flat or slightly raised irregularly colored patch with an asymmetric border, and it can arise in a preexisting nevus. The patch slowly expands peripherally and changes colors, revealing shades of tan, brown, blue, black, red, pink, or white over several years before become invasive.7 Absence of pigmentation within a superficial spreading melanoma often represents regression of the melanoma. This type of melanoma most characteristically meets the “ABCDE” criteria.1-3
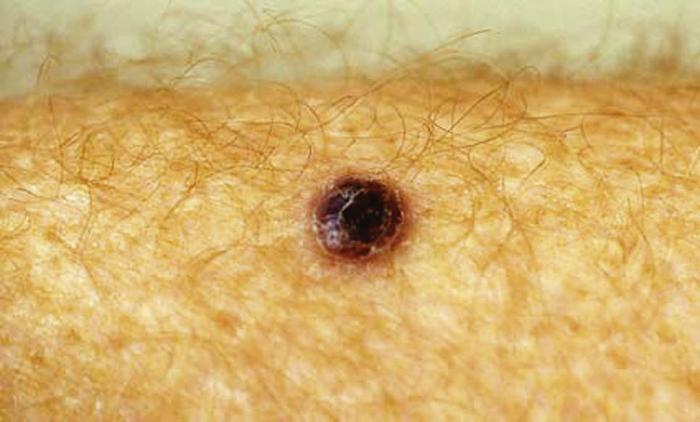
The second most common subtype of melanoma is nodular melanoma (Figure 5), the most rapidly growing and aggressive melanoma. Nodular melanoma represents 10% to 15% of all melanomas. Clinically, nodular melanoma manifests as a uniform blue-black, blue-red, or pink-red nodule. About 5% of nodular melanomas lack pigment (amelanotic melanoma). The most common sites are the trunk, head, and neck. It is more common for nodular melanoma to begin in normal skin rather than in a preexisting lesion. Nodular melanoma is usually invasive at the time of diagnosis.1-3
Acral lentiginous melanoma (Figure 6) is the least common type of melanoma in whites but are the most common type in Japanese, African Americans, Hispanics, and Native Americans. Unlike lentigo maligna melanoma, development of acral lentiginous melanoma does not seem to be associated with sun exposure. The median age for occurrence is 65, with equal sex distribution. Although these melanomas spread peripherally before invading deeper, there is often a delay in diagnosis because of the uncommon nature, with large, deep tumors at the time of presentation. Acral lentiginous melanoma usually appears as a black or brown discoloration on the palms or soles or under nails. The most common site of melanoma in African Americans is the feet, with 60% of patients having subungual or plantar lesions; the sole is the most common site in all races.1-3
Subungual melanoma (Figure 7) is a variant of acral lentiginous melanoma. Most subungual melanomas involve the great toe or thumb and generally arise from the nail matrix. The Hutchinson sign, the finding of pigmentation on the proximal nail fold as well as on the nail plate, is associated with advanced subungual melanoma. 1-3
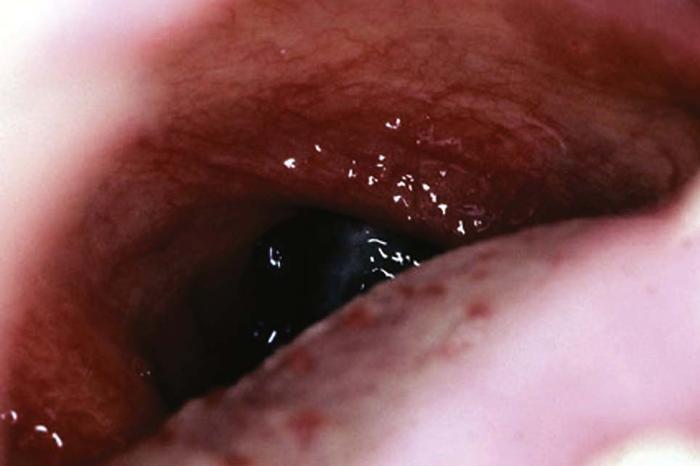
Mucosal melanoma (Figure 8) is another uncommon variant of melanoma, usually developing on the mucosal tissues of the head and neck (nasal and oral cavities) and the genital or anorectal mucosa. Patients can present with bleeding or a mass lesion. Melanoma can also present in the eye, associated with the retinal pigment epithelium.1-3
Desmoplastic melanoma (Figure 9) is a rare subtype of melanoma that is locally aggressive and has a high rate of local recurrence. It most commonly develops on sun-exposed skin of the head and neck of older adults. Desmoplastic melanoma has a male-to-female predominance of approximately 2 to 1. About half of desmoplastic melanomas develop in association with lentigo maligna. Desmoplastic melanoma can manifest clinically as a pigmented or skin-colored macule, papule, or nodule. Desmoplastic melanoma often invades perineurally and therefore is often symptomatic, with tingling or pain. In most cases, desmoplastic melanoma is deeply invasive (at least 5 to 6 mm thick) at the time of diagnosis.1-3
As with nonmelanoma skin cancers, biopsy is indicated for all suspicious pigmented lesions. Surface epiluminescence microscopy (dermatoscopy), in vivo reflectance confocal microscopy, and computer-aided multispectral objective evaluation are evolving adjunctive noninvasive diagnostic techniques that can aid clinical diagnosis and reduce unnecessary biopsies.20-22 Other noninvasive techniques are under development.
According to the American Academy of Dermatology (AAD) guidelines, the preferred biopsy technique is a narrow excisional biopsy that encompasses the entire breadth of the suspicious lesion with clinically negative margins, to a depth sufficient to ensure that the lesion is not transected by the base of the biopsy. This can be accomplished by “saucerization” shave removal, punch excision, or elliptical excision.7
Superficial shave biopsy, one of the most commonly performed procedures in dermatology clinics, remains controversial for the diagnosis of suspicious pigmented lesions. Some authors recommend shave biopsy, ensuring a depth of at least 1 mm of dermis, to reduce time to diagnosis, improve patient comfort by limiting invasiveness of the diagnostic procedure, and reduce scarring in the event of a nonmalignant biopsy result. Given the recommendation for sentinel lymph node biopsy (see below) for some thin and all intermediate-thickness melanomas, ensuring at least 1 mm of depth in the biopsy specimen allows patients to be appropriately referred for sentinel lymph node biopsy. However, as depth of invasion (Breslow thickness) has been proven to be the best prognostic indicator for melanoma, superficial shave biopsy in which the lesion is transected at the base of the biopsy specimen limits the clinician’s ability to accurately counsel patients on their disease, even if more than 1 mm of dermis is sampled.
Partial sampling of the thickest part of an atypical pigmented lesion with an incisional biopsy technique is appropriate when suspicion for melanoma is low, the lesion is large, or it is impractical to perform a complete excision (eg, facial or acral location). Repeat biopsy should be performed if the initial biopsy specimen is inadequate for accurate histologic diagnosis or staging. Fine-needle aspiration cytology should not be used to assess the primary tumor. Histologic interpretation should be done by a pathologist experienced in the microscopic diagnosis of pigmented lesions.7
Determining melanoma stage is important for planning appropriate treatment and assessing prognosis. The American Joint Committee on Cancer TNM (tumor, lymph node, metastasis) staging system breaks down the T classification based on the Breslow thickness; ulceration is classified as a high-risk feature for all tumors, and mitoses per mm2 is a high-risk feature for tumors with a thickness less than 1 mm.11
Sentinel lymph node biopsy is a diagnostic and therapeutic procedure to determine the presence or absence of metastatic melanoma cells in the draining nodal basin by removing the node that first receives and processes lymphatic fluid from the affected skin. Initially, lymphoscintigraphy is used to precisely map the draining nodal basin. A 1% isosulfan blue dye is injected around the cutaneous lesion to allow intraoperative localization of this sentinel lymph node. Alternately, a radioactive tracer (technetium-99) can be injected at the lesion site. A gamma probe is used to pinpoint the radiolabeled lymph node, which is then removed for histopathologic review.23
Determination of the status of the sentinel lymph node is relevant for several reasons. Sentinel node biopsy is a relatively low-risk procedure that can help identify high-risk patients who may benefit from additional therapy such as selective complete lymphadenectomy, adjuvant nivolumab or interferon alfa-2b, or radiation therapy. It also provides a psychological benefit for the patient whose biopsy does not reveal metastasis. Finally, the procedure may be associated with improved survival.24
According to the National Comprehensive Cancer Network (NCCN) [25], sentinel lymph node biopsy is important for staging but has not been shown to improve rates of disease-specific survival in all patients. Subset analysis of prospectively collected data from the Multicenter Selective Lymphadenectomy Trial 1 (MSLT-1) suggests that a negative sentinel lymph node biopsy is associated with improvement in the distant metastasis-free survival rate in patients with melanomas 1.2 to 3.5 mm thick, compared with patients with melanomas of similar thickness who are initially observed and subsequently develop clinical nodal metastasis.26
The MSLT-1 did not find a statistically significant melanoma-specific survival difference for patients who underwent sentinel lymph node biopsy compared with those who were observed, although biopsy was associated with a longer disease-free survival compared with observation.26
Additional studies have shown that only one-third of patients who develop metastatic disease are identified at the time of diagnosis via sentinel lymph node biopsy.25 In a large, single-institution survey, when lesions were stratified by Breslow thickness, no survival difference was found for patients with a negative biopsy compared with those with a positive biopsy. Lymph node status also did not demonstrate independent prognostic ability over Breslow thickness alone in multivariate analysis.27
The procedure is generally not recommended for in situ tumors or for stage I tumors with Breslow thickness ≤ 0.75 mm. Risk factors for a positive sentinel lymph node biopsy include ulceration, mitotic features, and lymphovascular invasion, but these are uncommon in lesions ≤ 0.75mm thick. If these risk factors are present, biopsy may be considered on an individual basis. For tumors with a Breslow thickness 0.76 to 1 mm without ulceration and with no mitoses per mm2, the NCCN guidelines recommend discussing and considering sentinel lymph node biopsy. For patients with clinically negative nodes with a primary tumor 0.76 to 1 mm thick with ulceration or any mitoses per mm2 or a tumor thicker than 1 mm, biopsy should be discussed and offered. Given the poor prognosis associated with thick melanoma, sentinel lymph node biopsy is controversial, although it remains a standard of care.25
The NCCN guidelines recommend imaging only to evaluate specific signs or symptoms in patients with in situ, stage I, and stage II disease. Imaging for baseline staging should be considered for patients with stage III disease with metastasis on sentinel lymph node biopsy, in addition to evaluating specific signs or symptoms. Baseline imaging for staging as well as investigating specific signs or symptoms is recommended in stage III disease with clinically palpable nodes, clinical satellitosis, or in-transit metastasis, as well as for all patients with stage IV disease.25
According to the NCCN guidelines, routine testing for BRAF is not indicated unless planning for systemic therapy.25 Gene expression profiling has been used to further stratify patients with localized, node-negative disease into high- and low-risk categories for the development of metastatic disease.28 Other internet-based nomograms have been developed to aid in developing a prognosis for individual patients.29-31
According to the AAD guidelines, the treatment of choice for primary cutaneous melanoma is surgical excision with histologic confirmation of tumor-free margins.7 This recommendation is also reflected in the NCCN guidelines.25 Excision should be to the depth of the deep subcutis for melanoma in situ and to the fascia for invasive melanoma. The recommended peripheral margins based on Breslow thickness are as follows:
In certain circumstances, surgical management needs to be tailored to the individual patient. Lentigo maligna may require margins much larger than 0.5 cm, given the propensity for broad subclinical extension; alternative techniques such as staged excision or Mohs micrographic surgery may be considered for complete peripheral and deep margin assessment.32 Invasive melanoma near a vital structure may require a reduced margin, and aggressive histologic features can suggest a more worrisome tumor and warrant a wider margin. Surgical excision at sites such as the fingers, toes, soles, and ears also need separate surgical considerations.
Mohs micrographic surgery for the treatment of melanoma remains controversial. The development of rapid immunostaining protocols has enabled several centers to routinely perform the procedure for melanoma, while other centers rely on permanent fixation for histology. Mohs micrographic surgery and margin-controlled excision of lentigo maligna offer lower recurrence rates and allow tissue to be conserved.32,33 Despite adequate surgical resection of the primary melanoma, 15% to 36% of patients with stages I and II melanoma have some form of recurrence or metastasis during their clinical course.
Completion lymph node dissection is defined as removing regional lymph nodes that drain the site of the primary melanoma in the presence of nodal metastases, including sentinel lymph node positivity, ultrasonographic findings, or clinically palpable disease. Completion lymph node dissection for nodal micrometastatic disease detected by positive biopsy study is a much-debated topic in the management of melanoma. The results of the Multicenter Selective Lymphadenectomy Trial II showed immediate completion lymph node dissection after positive sentinel lymph node biopsy was not superior to observation with routine nodal ultrasonography and delayed completion lymph node dissection in improving melanoma-specific survival rates, though there was increased disease control in the regional nodes and, thus, an improvement in disease-free survival.34 Treatment should be tailored to the individual, however, as patient-specific factors may warrant completion lymphadenectomy after a positive biopsy.
Interdisciplinary advances in the understanding of melanoma tumor biology and anti-tumor immunology over the past decade have translated into rapid advances in the treatment of melanoma that has spread beyond the skin [35]. Historically, treatment options for metastatic melanoma have offered only incremental improvements in survival. Newer treatments have offered patients with metastatic melanoma the chance for durable disease-free survival and, in some cases, a cure. Additionally, patients with localized melanoma who are at high risk of developing metastatic disease may be treated with these newer agents.
As discussed above, activating mutations in BRAF are common in melanoma. Two agents, vemurafenib and dabrafenib, are approved by the US Food and Drug Administration (FDA) for the treatment of tumors with the characteristic V600E mutation. In single-agent clinical trials, both medications have been shown to provide significant improvements in progression-free survival rates compared with dacarbazine. Vemurafenib was also associated with a statistically significant improvement in overall survival; dabrafenib treatment showed a trend to increased overall survival, but the trend was not statistically significant. Both agents also have activity against brain metastases.36,37
Initial optimism over these medications was tempered somewhat by the fact that most patients treated with single agent BRAF inhibitors eventually have disease progression. Consequently, multi-agent treatment strategies combining BRAF inhibition with another targeted treatment have largely replaced single-agent regimens.
Multiple mutations develop within tumors after single-agent BRAF inhibition is initiated, re-activating the aberrant MAP kinase pathway, thus leading to resistance to the medications and to disease progression. Several mutations were identified that give tumor cells a survival advantage, including several substitution mutations in MEK1.
Trametinib is an MEK inhibitor FDA-approved as single-agent therapy for advanced melanoma; cobimetinib has been approved for use in combination with vemurafenib for patients with a BRAF V600E mutation. Compared with chemotherapy, trametinib significantly lengthened progression free survival and overall survival,38 and combination cobimetinib-vemurafenib therapy lengthened progression-free survival and median survival compared with chemotherapy.39
In the COMBI-AD trial [40], combination BRAF-MEK inhibition was studied as adjuvant therapy for melanoma. Dabrafenib-trametinib combination therapy in patients with BRAF mutant stage III melanoma reduced the risk of disease recurrence or death by 53% compared with placebo after 3 years. Preliminary data revealed an increased rate of overall survival, 77% in the placebo arm vs 86% in the treatment arm.40 As a result of the study, dabrafenib-trametinib was approved as an adjuvant treatment for patients with BRAF V600E- or V600K-positive melanoma.
Mutations of the NRAS gene were also discovered in a study of patients who developed resistance to single-agent BRAF inhibitors. Binimetinib is an MEK inhibitor that has activity against melanoma with a mutation in NRAS. At the time of this writing, it is still in clinical trials and has not been approved for use outside a clinical trial setting.
Mutations in cKIT are infrequently identified in patients with acral, mucosal, or cutaneous melanoma in the setting of chronic sun damage. KIT inhibitors, including imatininb and nilotinib, have been studied more in patients with mucosal melanoma rather than primary cutaneous melanoma. Although small trials have not shown KIT inhibitors to be significantly effective, patients with mutations in exon 11 or 13 of the KIT gene seem to respond to KIT inhibitors.41,42 At the time of this writing, no KIT inhibitors have been approved for patients outside a clinical trial setting.
As our understanding of melanoma tumor biology has allowed for rapid deployment of targeted therapies against melanoma, so too have steady advances in tumor immunology. Specifically, the discovery of immune checkpoints, considered the “breakthrough of the year” in 2013,43 has led to the development of several drugs approved for patients with stage III or IV melanoma. Immune checkpoint inhibitors increase antitumoral immunity by blocking the interaction of tumor cell antigens with activated T cells. These medications prevent tumor cells from inactivating T cells via either cytotoxic T-lymphocyte antigen 4 (CTLA-4) or programmed cell death receptor 1 (PD-1). Interestingly, patients treated with immune checkpoint inhibitors may experience disease progression before they respond; however, patients with early rapidly progressive disease generally do not subsequently respond.
Ipilimumab has demonstrated prolonged overall survival in large clinical trials, with a prolonged survival b enefit for those patients who respond well to treatment. In patients with metastatic melanoma who were not treated with other agents, ipilimumab plus dacarbazine outperformed placebo plus dacarbazine in overall survival. Additionally, in paients previously treated with chemotherapy or interleukin-2, treatment with ipilimumab significantly increased overall survival and objective response rate.44 Across all trials, the minority of patients who have a complete response seem to have a long survival: 22% of patients who were followed for at least three years survived and 21% survived to ten years.45
Ipilimumab is approved for adjuvant therapy after surgical excision of high-risk melanomas. However, ipilimumab has become a second-line agent for adjuvant therapy for high-risk melanoma as well as primary immunotherapy for metastatic melanoma because of the improved efficacy and tolerability of PD-1 inhibitors.
Pembrolizumab was compared with chemotherapy in patients refractory to ipilimumab in the KEYNOTE 002 study. In this phase 2 study, patients treated with pembrolizumab had longer progression-free survival as well as a higher objective response rate compared with patients treated with chemotherapy.46 Additionally, in the KEYNOTE 006 trial, compared with ipilimumab treatment, pembrolizumab resulted in significantly improved progression-free survival, overall survival, and objective response rate.47
Nivolumab has been proven effective as both a single agent and in combination with ipilimumab. In the CheckMate 066 trial, nivolumab was compared with dacarbazine in patients not previously treated. Nivolumab led to significantly increased overall survival, progression-free survival, and objective response rate [48]. Also, in the CheckMate 037 trial, nivolumab was compared with chemotherapy in patients previously treated with ipilimumab and a BRAF inhibitor, if appropriate. In this trial, overall survival rates were not significantly different; however, objective responses were more common and the median duration of response was longer in patients treated with nivolumab.49
Ipilimumab and nivolumab were studied together against either ipilimumab or nivolumab in the CheckMate 067 trial. Combination therapy was associated with improved progression-free survival, overall survival, and objective response rate compared with ipilimumab alone. Unfortunately, the trial did not have suitable power to compare the combination treatment against nivolumab alone.50 Nivolumab is also approved for adjuvant therapy and for treatment of patients with stage III melanoma.
In the Eastern Cooperative Oncology Group (ECOG) 1684 study, high-dose interferon alfa-2b was initially reported to improve survival rates in patients with melanoma lesions thicker than 4 mm;51 however, the follow-up trial ECOG 1690 did not show an overall survival benefit.52 Another major study reported by the Austrian Malignant Melanoma Cooperative Group did show that adjuvant treatment with low-dose interferon alfa-2b decreased the occurrence of metastases and prolonged the disease-free survival in patients with melanoma lesions thicker than 1.5 mm.53
Interleukin-2 (IL-2) as a single agent has been used in metastatic melanoma. In one study, 7% of patients had a complete response that was durable: patients remained disease-free for up to 8 years after initiation of therapy.54
Systemic chemotherapy is used primarily for melanoma that is advanced stage III (unresectable regional metastases) or stage IV (distant metastases). Although chemotherapy is generally not effective, dacarbazine remains the only FDA-approved chemotherapeutic agent for treating advanced melanoma in the United States. The response rate is in the range of 10% to 20%, and patients with metastases in the skin, subcutaneous tissues, or lymph nodes respond most often. Other combination chemotherapy and biochemotherapy regimens could achieve higher response rates but do not appear to lead to durable remission.55,56
Talimogene laherparepvec (T-VEC) is a genetically modified herpes simplex type 1 virus that selectively destroys tumor cells by replicating within the tumor cells and by inciting the host immune response against the tumor by producing granulocyte-monocyte colony stimulating factor (GM-CSF). It is FDA-approved for intralesional injection into nonresectable cutaneous, subcutaneous, or nodal lesions in patients with metastatic melanoma with limited systemic disease. In clinical trials, compared with administration of GM-CSF alone, T-VEC produced significantly increased rates of response lasting longer than 6 months, although overall survival was only prolonged for patients with stage III and IVa disease. Patients with M1b or M1c disease did not have an overall survival benefit.57
Other injectable therapies under development include HLA-B7 gene therapy and PV-10.
Historically, melanoma was considered to be radio-resistant, with limited applications. However, methods of delivering radiation therapy have improved, and it is indicated in multiple settings for patients with melanoma. Limited metastatic disease can be ablated with stereotactic radiosurgery; in one study, more than 85% of tumors smaller than 1 cm completely responded to a course of radiation therapy.58 Primary treatment of melanoma with radiation alone or after an initial, inadequate excision should be reserved for carefully selected tumors after discussion with the patient.
Radiation therapy has been used locally after excision of a primary melanoma with high-risk features (eg, desmoplastic tumor) to reduce the rate of local recurrence. For patients with a high risk of nodal metastasis who are unable to undergo sentinel lymph node biopsy, radiation can be delivered to the nodal basin to reduce the rate of lymphatic disease. In the presence of nodal metastasis, radiation has been used as adjuvant therapy after lymphadenectomy for regional nodal disease.59
Given the advances in targeted therapies and immunotherapies, radiation therapy is reserved for certain patients with stage IV disease. It can be used for consolidation in patients not achieving a complete response to systemic therapy. It is often used as palliative therapy for patients who develop unresectable, locally recurrent, or symptomatic metastatic disease. Specific indications include brain metastases or central nervous system symptoms, pain associated with bone metastases, spinal cord compression, and superficial skin and subcutaneous metastases.
Isolated limb perfusion with melphalan has been used as adjuvant treatment or as treatment of locally recurrent melanoma of an extremity. In isolated limb perfusion, the limb is isolated from the systemic circulation with a tourniquet, using arteriovenous bypass. Melphalan is infused via a pump oxygenator, and then the medication is removed from the limb. In some cases, the limb is first heated to above the normal physiologic temperature (“hyperthermic” isolated limb perfusion). The procedure is effective for local recurrent or in-transit metastases of an extremity.26 Medications used for infusion other than melphalan include dacarbazine, cisplatin, carboplatin, thiotepa, and cytokine tumor necrosis factor alpha.60
Approximately 85% of patients with melanoma have localized disease (stages I and II) at presentation, about 15% have regional nodal disease, and only about 2% have distant metastases at the time of diagnosis.1-3 The prognosis for stage I and II melanoma can be affected by many factors. Clinical factors associated with a favorable prognosis include younger age, female sex, and extremity lesions. Increasing Breslow thickness is the most important negative prognostic indicator, with worse survival for every stratum of tumor thickness in the American Joint Committee on Cancer staging guidelines. Other histologic variables associated with a poor prognosis include ulceration, diminished lymphoid response, evidence of tumor regression, microscopic satellites, lymphovascular invasion, and non–spindle-cell type tumors.25
The presence of regional lymph node metastases imparts an overall 5-year melanoma-specific survival rate of 77% and a 10-year melanoma-specific survival of 69%. When adjusting for size of lymph node deposits and number of nodes involved, the melanoma-specific survival ranges from 57% to 82% at 5 years and 47% to 75% at 10 years.11 The most important prognostic factor for stage III melanoma is the number of positive lymph nodes. Patients with nodal micrometastases have an improved survival compared with patients with clinically palpable nodes. Patients with melanoma on an extremity and younger age at diagnosis have been shown to have a better prognosis. If there are distant metastases, median survival is about 6 to 9 months.1-3, 11, 61 For stage IV, the prognostic variables suggesting worse prognosis include increasing number of metastatic sites, visceral location of metastases (lung, liver, brain, bone), absence of resectable metastases, male sex, and shorter duration of remission.1-3, 11, 61 Patients with nonvisceral disease (eg, skin, subcutaneous tissue, lymph nodes) have a better median survival rate, ranging from 12 to 15 months, and are more likely to respond to chemotherapy.61
In order to offer the best counseling to patients, all data related to the tumor must be synthesized into as precise a stage as possible. The revised TNM staging as proposed by the American Joint Committee on Cancer is presented in Table 1.11
Primary tumor (T)
| ||
|---|---|---|
| T category | Thickness | Ulceration status |
| TX: Primary tumor thickness cannot be assessed (eg, diagnosis by curettage) | Not applicable | Not applicable |
| T0: No evidence of primary tumor (eg, unknown primary or completely regressed melanoma) | Not applicable | Not applicable |
| Tis (melanoma in situ) | Not applicable | Not applicable |
| T1 | ≤ 1.0 mm | Unknown or unspecified |
| T1a | < 0.8 mm | Without ulceration |
| T1b | < 0.8 mm | With ulceration |
| 0.8 to 1.0 mm | With or without ulceration | |
| T2 | > 1 to 2 mm | Unknown or unspecified |
| T2a | > 1 to 2 mm | Without ulceration |
| T2b | > 1 to 2 mm | With ulceration |
| T3 | > 2 to 4 mm | Unknown or unspecified |
| T3a | > 2 to 4 mm | Without ulceration |
| T3b | > 2 to 4 mm | With ulceration |
| T4 | > 4 mm | Unknown or unspecified |
| T4a | > 4 mm | Without ulceration |
| T4b | > 4 mm | With ulceration |
| Regional lymph nodes (N) | ||
| N category | Extent of regional lymph node and/or lymphatic metastasis |
|
| Number of tumor-involved regional lymph node | Presence of in-transit, satellite, and/or microsatellite metastases | |
| NX | Regional nodes not assessed: eg, sentinel lymph node (SLN) biopsy not performed, regional nodes previously removed for another reason Exception: Pathologic N category is not required for T1 melanomas, use clinical N information |
No |
| N0 | No regional metastases detected | No |
| N1 | One tumor-involved node or in-transit, satellite, and/or microsatellite metastases with no tumor-involved nodes | |
| N1a | One clinically occult (ie, detected by SLN biopsy) | No |
| N1b | One clinically detected | No |
| N1c | No regional lymph node disease | Yes |
| N2 | Two or three tumor-involved nodes or in-transit, satellite, and/or microsatellite metastases with one tumor-involved node | |
| N2a | Two or three clinically occult (ie, detected by SLN biopsy) | No |
| N2b | Two or three, at least one of which was clinically detected0 | No |
| N2c | One clinically occult or clinically detected | Yes |
| N3 | Four or more tumor-involved nodes or in-transit, satellite, and/or microsatellite metastases with two or more tumor-involved nodes, or any number of matted nodes without or with in-transit, satellite, and/or microsatellite metastases | |
| N3a | Four or more clinically occult (ie, detected by SLN biopsy) | No |
| N3b | Four or more, at least one of which was clinically detected, or presence of any number of matted nodes | No |
| N3c | Two or more clinically occult or clinically detected and/or presence of any number of matted nodes | Yes |
| Distant metastasis (M)) | ||
| M category | M criteria |
|
| Anatomic site | LDH level | |
| M0 | No evidence of distant metastasis | Not applicable |
| M1 | Evidence of distant metastasis | See below |
| M1a | Distant metastasis to skin, soft tissue including muscle, and/or nonregional lymph node | Not recorded or unspecified |
| M1a(0) | Not elevated | |
| M1a(1) | Elevated | |
| M1b | Distant metastasis to lung with or without M1a sites of disease | Not recorded or unspecified |
| M1b(0) | Not elevated | |
| M1b(1) | Elevated | |
| M1c | Distant metastasis to non-central nervous system (CNS) visceral sites with or without M1a or M1b sites of disease | Not recorded or unspecified |
| M1c(0) | Not elevated | |
| M1c(1) | Elevated | |
| M1d | Distant metastasis to CNS with or without M1a, M1b, or M1c sites of disease | Elevated |
| M1d(0) | Not elevated | |
| M1d(1) | Elevated | |
Source: Adapted from reference 11.
All data related to the tumor can be used to group patients into one of several clinical stages, as shown in Table 2 .11 Clinical staging includes histologic data related to the primary tumor in addition to information from the clinical and radiologic evaluation for metastatic disease. Conventionally, clinical staging should be used after biopsy of the primary tumor, with clinical assessment for regional and distant metastases. As such, there is only 1 clinical stage for lymph node metastases and 1 stage for distant metastases. Pathologic assessment of the primary melanoma is used for both clinical and pathologic classification. A diagnostic evaluation of regional and distant metastases is included. Pathologic staging includes histologic information related to the primary tumor from biopsy and excision, and information about the regional lymph nodes after sentinel lymph node biopsy or completion lymph node dissection for clinically evident regional lymph node disease.
Clinical tumor, node, metastasis (cTNM)
| |||
|---|---|---|---|
| When T is... | And N is... | And M is... | Then the clinical stage group is... |
| Tis (melanoma in situ) | N0 | M0 | 0 |
| T1a | N0 | M0 | IA |
| T1b | N0 | M0 | IB |
| T2a | N0 | M0 | IB |
| T2b | N0 | M0 | IIA |
| T3a | N0 | M0 | IIA |
| T3b | N0 | M0 | IIB |
| T4a | N0 | M0 | IIB |
| T4b | N0 | M0 | IIC |
| Any T, Tis | ≥ N1 | M0 | III |
| Any T | Any N | M1 | IV |
Pathologic (pTNM)
| |||
| When T is... | And N is... | And M is... | Then the pathologic stage group is... |
| Tis | N0a | M0 | 0 |
| T1a | N0 | M0 | IA |
| T1b | N0 | M0 | IA |
| T2a | N0 | M0 | IB |
| T2b | N0 | M0 | IIA |
| T3a | N0 | M0 | IIA |
| T3b | N0 | M0 | IIB |
| T4a | N0 | M0 | IIB |
| T4b | N0 | M0 | IIC |
| T0 | N1b, N1c | M0 | IIIB |
| T0 | N2b, N2c, N3b, or N3c | M0 | IIIC |
| T1a/b-T2a | N1a or N2a | M0 | IIIA |
| T1a/b-T2a | N1b/c or N2b | M0 | IIIB |
| T2b/T3a | N1a-N2b | M0 | IIIB |
| T1a-T3a | N2c or N3a/b/c | M0 | IIIC |
| T3b/T4a | Any N ≥ N1 | M0 | IIIC |
| T4b | N1a-N2c | M0 | IIIC |
| T4b | N3a/b/c | M0 | IIID |
| Any T, Tis | Any N | M1 | IV |
a Pathologic stage (melanoma insitu) and T1 do not require pathologic evaluation of lymph nodes to complete pathologic staging; uses clinical N information to assign the pathologic stage.
Source: Adapted from refernce 11.
The prognosis for a patient with localized primary cutaneous melanoma is mainly related to tumor thickness. Survival data for patients with nodal status known to be negative is shown in Table 3.11
| T category | 5-year survival | 10-year survival |
|---|---|---|
| T1b | 99% | 96% |
| T2a | 96% | 92% |
| T2b | 93% | 88% |
| T3a | 94% | 88% |
| T3b | 86% | 81% |
| T4a | 90% | 83% |
| T4b | 82% | 75% |
Source: Adapted from refernce 11.
Note: Thickness is defined as the thickness of the lesion using an ocular micrometer to measure the total vertical height of the melanoma from the granular layer to the area of deepest penetration. The Clark level refers to levels of invasion according to depth of penetration of the dermis.
Prognosis for patients with nodal disease relates to both thickness of the primary tumor, the size and extent of metastatic deposits within the lymph node, and presence of distant metastases. The 5- and 10-year survival data for patients with known metastatic disease in the lymph node is presented in Table 4.11
| Nodal status (N) | 5-year survival | 10-year survival |
|---|---|---|
| N1 | 82% | 75% |
| N1a | 84% | 75% |
| N1b | 76% | 71% |
| N1c | 81% | 75% |
| N2 | 76% | 68% |
| N2a | 79% | 71% |
| N2b | 71% | 71% |
| N2c | 69% | 59% |
| N3 | 57% | 47% |
| N3a | 60% | 46% |
| N3b | 64% | 57% |
| N3c | 52% | 43% |
Source: Adapted from refernce 11.
Melanoma specific survival data, when combining staging data for the primary tumor, nodal disease, and the presence or absence of distant metastases, is presented in Table 5.11
| 5-year survival | 10-year survival | |
|---|---|---|
Clinical stage |
||
| IA | 99% | 98% |
| IB | 97% | 94% |
| IIA | 94% | 88% |
| IIB | 87% | 82% |
| IIC | 82% | 75% |
| III | ||
| IV | ||
Pathologic stage |
||
| IIIA | 93% | 88% |
| IIIB | 83% | 77% |
| IIIC | 69% | 60% |
| IIID | 32% | 24% |
| IV | 15% | 12% |
Source: Adapted from refernce 11.
The goal of regular follow-up of patients with melanoma is the detection of local recurrence, regional metastasis to lymph nodes, distant metastasis of the primary melanoma, or development of a second primary melanoma. Each visit should include a detailed history and physical examination, with further testing driven by specific signs and symptoms. For most patients with stage I or II melanoma, follow-up appointments should be scheduled every 3 months for the first 2 years, then every 6 months for 3 years, then once a year thereafter. If the patient has dysplastic nevi, the interval may be continued at every 6 months indefinitely.
Given the results of the Multicenter Selective Lymphadenectomy Trial II,34 patients with stage III melanoma who have occult disease detected only with sentinel lymph node biopsy may be followed with serial ultrasonography of the regional basin, rather than immediate completion lymph node dissection. The optimal interval for sonographic evaluation has not been determined, although a similar interval can be used as suggested above for patients with stage I or II disease.
Clinical serial photography may be helpful when following patients with multiple clinically atypical nevi. Patients should also be taught and encouraged to practice monthly skin self-examination. Because most experts attribute the rising trend in the overall 5-year melanoma survival rate (from 40% in the 1940s to the current rate of 86%) to improved early detection, it is very important for physicians and the public to be aware of the early warning signs of melanoma and to get appropriate dermatologic evaluation and treatment as soon as possible.
Many new technologies are being developed to help clinicians and patients evaluate moles. These include handheld and computer-aided epiluminescence microscopy and ultrasound-based devices, as discussed above. Additionally, smartphone applications have been developed to store clinical photographs and enable patients to evaluate changes in their moles over time. Finally, smartphone and office-based teledermatology platforms are proving to shorten the time to diagnosis by reducing barriers to specialty care.
Primary prevention of melanoma requires reduction of known risk factors in people at risk. The most important modifiable behavior for melanoma prevention is reduction of ultraviolet exposure, both from the sun and from tanning beds. Educating the public about sun avoidance and sun protection, risk factors for developing skin cancer, and skin self-examination is essential.62 AAD skin cancer awareness initiatives such as “Melanoma Monday”—an annual national event offering free skin cancer screening conducted by dermatologists to raise awareness about melanoma and encourage a lifelong habit of regular skin examination—and “Sun Smart” have been particularly effective in changing our society's approach to the sun.1-3 , 62
The author would like to thank Rebecca Tung, MD, and Allison Vidimos, MD, for their previous work in developing this chapter.