Published: March 2017
Colorectal cancer (CRC) is the third most common cancer and the third leading cause of cancer–related deaths in the United States. It is estimated that approximately 135,000 new cases of CRC will be diagnosed in 2016 and that 50,000 deaths from colorectal cancer will occur.1 CRC screening has been associated with a decrease in CRC incidence and mortality.2 Unfortunately, only 65% of eligible Americans are up–to–date with the recommended screening. Colorectal cancers detected on screening are more likely to be early stage and curable compared with cancers detected on an examination done for symptoms related to the tumor. Efforts should be focused on improving the rates of screening, recognizing and mitigating risk factors, adhering to evidence based intervals for colonoscopic surveillance, and enhancing the quality of colonoscopy.
Three well–established molecular pathways, the chromosomal instability (CIN), microsatellite CpG island methylator phenotype (CIMP), and microsatellite instability (MSI), have broadened our understanding of the pathogenesis of CRC. The majority of CRCs arise through the CIN pathway where by genetic alterations including loss of heterozygosity and progressive mutations occur as the adenomas progress to cancer. The activation of oncogenes (eg, Kirsten rat sarcoma [K–ras] KRAS, c–src and c–myc) and deactivation of tumor suppressor genes (eg, APC and p53) result in unchecked cellular proliferation and disordered apoptosis.3 Over time, the affected cells continue to accumulate mutations, often altering the total number of chromosomes, until they transform into an adenoma and eventually invasive adenocarcinoma.
Up to 30% of CRCs arise from sessile serrated polyps (SSP) through the CIMP pathway. The primary cause of cellular dysfunction in this pathway occurs through epigenetic or acquired modification to genes through methylation of the CG–rich promoter regions, which effect gene expression and function. Two commonly affected genes in the SSP–CRC pathway include mutations in the oncogene BRAF and methylation of the DNA mismatch repair gene MLH1.
The third pathway is characterized by defects in the DNA mismatch repair (MMR) apparatus, leading to replication errors in areas of the genome containing simple repeated nucleotide sequences, called MSI.4 CRCs that have evidence of MSI may be the result of a germline mutation in one of the MMR genes, which is the sine qua non of Lynch Syndrome, due to bi–allelic somatic genetic alterations in the tumor MMR genes or due to tumor methylation of MLH1, which is a hallmark of CRCs arising from SSPs.
CRC arises from neoplastic epithelial polyps including adenomatous and sessile serrated polyps. The most common precancerous colon polyp is the adenoma, which is believed to be the precursor for about 80% of CRC. Studies of individuals of average risk of CRC and 50 years and older found 22% to 42% harbor adenomas.5
Adenomatous polyps can be further classified by histologic features (tubular, tubulovillous, and villous) and the degree of dysplasia (low grade and high grade). Strong evidence demonstrates that the polyp features most strongly associated with the future risk of an advanced adenoma or CRC include large size (≥10 mm), number of polyps (>2), high-grade dysplasia and presence of villous features in the polyp (Table 1).6-8
| Baseline adenoma feature | Odds ratio (95% CI) |
|---|---|
| 2 adenomas vs 1 adenoma | |
| 3 adenomas vs 1 adenoma | |
| 4 adenomas vs 1 adenoma | |
| Proximal vs distal | |
| 5–9 mm vs <5 mm | |
| 10–19 mm vs <5 mm | |
| Tubulovillous/villous vs tubular |
CI = confidence interval.
Data from Martinez et al.6.
Serrated polyps are those that have a saw tooth appearance microscopically. The 3 types of serrated polyps of the colon include the hyperplastic polyp (HP), sessile serrated adenoma (SSP), and the traditional serrated adenoma (TSA). SSPs are believed to be the precursor to CRC in 20% to 35% of the cases and are detected in 2% to 10% of patients undergoing average risk screening colonoscopy.9,10 Their molecular characteristics include high levels of CIMP, a v600E BRAF mutation, and MSI due to methylation of MLH1.4,11 They are often in the proximal colon, flat and difficult to detect. The distinction between SSPs and HPs is based upon the morphology of the glandular epithelial crypt base. Hyperplastic polyps are the most common serrated polyp and are found in about 25% of patients. They are most often small, and primarily found in the rectum and sigmoid. The small HPs in the recto–sigmoid colon are not believed to have malignant potential. Traditional serrated adenomas are very rare (<1%) neoplasms, usually in the left colon and are molecularly and phenotypically similar to conventional adenomas.
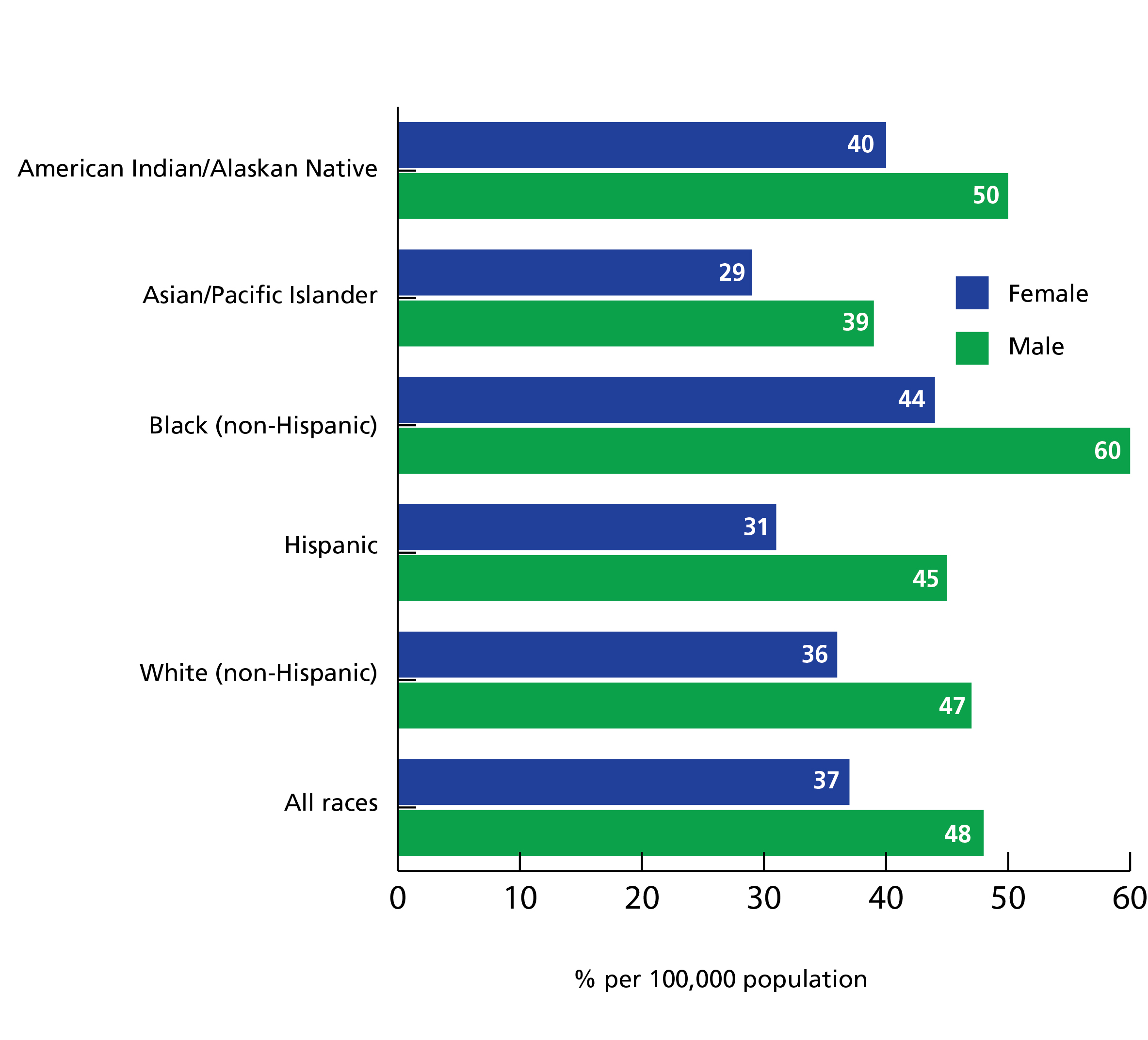
Men and women in the U.S. face a lifetime risk of developing CRC of nearly 5% (Table 2).1 Over 90% of cases occur in individuals older than 50 years.2 Black men and women have the highest incidence of CRC and stage–adjusted CRC mortality (Figure 1).1 The lowest incidence of CRC occurs among Asians/pacific islanders and in all races and ethnic groups, the incidence is lower in women compared with men.1 The prevalence of adenomas and CRC is about one–third higher in men than in women; the cause of this is unclear, however an interplay between sex–specific predisposition to DNA–methylation in colonic mucosa, varying hormonal levels, and exposure to dietary and lifestyle risk factors such as red meat and alcohol consumption, smoking, and physical activity may be factors.12 Interestingly, incidence rates also vary by geographic location in the U.S. with the highest rates in the Northeast and lowest in the Southwest and may be partly attributed to sun exposure and Vitamin D levels.13
| Birth to 49 years, % | 50–59 years, % | 60–69 years, % | 70 years and older, % | Birth to death, % | |
|---|---|---|---|---|---|
| Male | 0.3 (1 in 300) | 0.7 (1 in 149) | 1.2 (1 in 82) | 3.7 (1 in 27) | 4.7 (1 in 21) |
| Female | 0.3 (1 in 318) | 0.5 (1 in 195) | 0.9 (1 in 117) | 3.4 (1 in 30) | 4.4 (1 in 23) |
aUS population, 2010–2012.
Data from Siegel et al.1
Epidemiologic studies have implicated a number of factors associated with an increased risk of CRC including an unhealthy diet and lifestyle, black race, advanced age, chronic colitis and a personal and family history of colorectal polyps and CRC (Table 3).14-16 The greater the number and younger age of relatives with polyps or CRC, and the closeness of the familial relationship affects an individual's risk of CRC.17,18
| Risk factor | Relative risk (95% CI) |
|---|---|
| Alcohol: heavy (140–257 g/week) vs non-drinker | |
| Obesity: BMI ≥30 vs ≤25 | |
| Smoking: current vs never smoker | |
| Diabetes | |
| Red meat consumption (100 g/day increase) | |
| Processed meat consumption (50 g/day increase) |
CI = confidence interval; BMI = body mass index.
aData from Huxley et al.14
bData from Yuhara et al.15
cData from Chan et al.16.
Individuals at highest risk for CRC are those with a hereditary CRC syndrome due to a germline gene mutation. Nearly all of the hereditary CRC syndromes are inherited in an autosomal dominant fashion and account for approximately 10% of the CRC cases. The most common CRC syndromes include familial adenomatous polyposis (FAP), MYH-associated polyposis (MAP) and Lynch syndrome. Patients and families with hereditary CRC syndromes should undergo genetic counseling and genetic testing and adhere to recommended guidelines for intensive cancer surveillance and prophylactic surgery.19,20
Familial adenomatous polyposis is caused by a mutation in the tumor suppressor gene APC. By the second decade of life, individuals with FAP develop hundreds to thousands of colorectal adenomas. CRC develops in nearly all patients with FAP by age 40 years if prophylactic colectomy is not performed. In individuals with the subtype attenuated FAP (AFAP),fewer colonic polyps (usually less than 100) occur polyposis occurs at a later age, and the lifetime risk of CRC is lower than individuals with FAP The extracolonic manifestations of FAP/AFAP include duodenal adenomas associated with periampullary cancer, thyroid cancer, gastric polyposis and gastric cancer, benign soft tissue tumors (lipomas, fibromas, sebaceous cysts), osteomas, supernumerary teeth, adrenal adenomas, desmoid tumors, and congenital hypertrophy of the retinal pigment epithelium.
MAP is caused by biallelic mutations of the MYH gene and is inherited in an autosomal recessive fashion. Individuals with MAP have a 19% risk of CRC presenting by the age of 50 with a colorectal polyp phenotype mimicking attenuated FAP. The extra–colonic manifestations of MAP are similar although less prevalent than FAP.
Lynch syndrome (LS) is defined as an individual who carries a germ-line mutation in one of the four DNA mismatch repair genes or the EPCAM gene. The lifetime risk of CRC is reported to be up to 74% though varies by genotype and can be mitigated by colonoscopy surveillance. Endometrial, ovarian, small bowel, urothelial, skin, gastric and brain cancer occur in patients with LS. Early onset and frequent screening for endometrial and ovarian cancers and prophylactic total hysterectomy and bilateral salpingo-oopherectomy is recommended for women with LS. Historically, the diagnosis of LS was based upon the Amsterdam Criteria I and II and the revised Bethesda criteria.20 The criteria do not have sufficient diagnostic sensitivity or specificity for the identification of patients with LS. Since MSI is the hallmark of CRC due to LS, testing all patients with CRC for evidence of MSI or MMR deficiency, known as universal testing, is currently recommended to assist in identifying patients who may have LS.20
Chronic colonic inflammation due to inflammatory bowel disease (IBD) including ulcerative colitis and Crohn’s disease is associated with an increased risk of CRC. The risk is related to the anatomic extent of affected colon (above the sigmoid colon), severity of inflammation, and duration of disease (>8 years).21 Concurrent primary sclerosing cholangitis (PSC) and IBD is a strong risk factor for CRC with a nearly fivefold increased risk compared with patients with IBD without PSC.22
The incidence of CRC has significantly decreased in the last 3 decades in adults over the age of 50 years, mainly attributed to an increased CRC screening. Several professional societies have recommendations on colorectal cancer screening. The U.S. Preventive Services Task Force (USPSTF) has recently published updated CRC screening guidelines endorsing a variety of available screening modalities for individuals aged 50 to 75 years (Table 4).23 Individuals aged 76 to 85 years who have previously been screened derive less benefit than those who have never been screened. Thus screening those 76 to 85 years of age who have been previously screened and individuals less than 50 years should be an individualized decision. The American College of Gastroenterology recommends screening at the age of 45 in African Americans because of the increased incidence and earlier age of onset of CRC in this population.24
Available screening tests can be divided into those that detect cancer and those that prevent CRC by detection and treatment of precancerous colonic lesions. High quality colonoscopy is often recommended as the preferred screening modality. Advantages include a long interval between normal exams, direct mucosal visualization, and ability to remove lesions.
| Method | Screening Interval |
|---|---|
| High sensitivity gFOBT or FIT | |
| Stool DNA | |
| Computed tomography colonography | |
| Flexible sigmoidoscopy | |
| Colonoscopy |
gFOBT = guaiac fecal occult blood test; FIT = fecal immunochemical test.
Data from U.S. Preventive Services Task Force.23.
Fecal occult blood tests (FOBTs) detect bleeding from large adenomas and CRC. There are 2 types of FOBTs, a guaiac–based test and an immunochemical-based test. Guaiac FOBTs (gFOBT) take advantage of the peroxidase activity of hemoglobin that can be detected in the stool by a color change when it catalyzes the oxidation of guaiac by a peroxide reagent. Three randomized controlled trials found that the use of annual gFOBTs decreased the mortality from CRC by up to 33% compared with unscreened patients.25 In a trial of 46,551 participants aged 50 to 80 years through 30 years of follow–up, annual screening and biannual screening to a lesser extent reduced the risk of dying from CRC compared with usual care.26 The only gFOBT approved by the U.S. Food & Drug Administration (FDA) is the Hemoccult Sensa (Beckman Coulter). Pseudoperoxidases in foods may cause false positive guaiac tests; therefore, a special diet (eg, meat–free, high–residue diet without vegetables with peroxidase activity such as turnips and horseradish) is recommended for at least 24 hours before 3 separate stool specimens are collected each 1 day apart. The USPSTF guidelines endorse an option of high sensitivity gFOBT annually. Any individual with a positive gFOBT test should be evaluated with a colonoscopy.
Immunochemical–based FOBTs, known as fecal immunochemical tests (FIT) use antibodies to human globin to detect blood in the stool. The advantage of the FIT includes an increase in compliance as only one sample is needed and no dietary restrictions are required because FIT antibodies do not cross–react with nonhuman hemoglobin or peroxidase from food sources. Hemoglobin does not survive passage through the upper gastrointestinal tract, therefore the test is specific for colorectal bleeding. FIT can be both qualitative and quantitative. The fecal hemoglobin threshold for a positive test can be altered. When a cutoff of ≥75 ng/mL is used, the CRC detection sensitivity is 94% and the specificity is 87.5% and the clinically significant neoplasm sensitivity is 67% and the specificity is 91.4%.
FIT has been shown in case–control studies to reduce CRC mortality of up to 80%. A large retrospective study demonstrated that programmatic annual FIT testing in an organized health system remained highly sensitive at 78% for CRC over 4 years of screening. Adherence to annual FIT in the 48% of participants participating in the first round of screening ranged from 75% to 86% over the screening period.28
The accuracy of a one–time FIT for the detection of CRC and advanced adenomas is higher than with gFOBT. CRC sensitivity with FIT has been reported to be 87.5% and 82% compared with gFOBT reported to be 54.2% and 64.3%.29,30 The sensitivity for the detection of advanced adenomas is nearly double with FIT at 42.6% versus 23% for gFOBT.29 The specificity of each modality is greater than 98%. Annual FIT is endorsed by the USPSTF. Any positive test should be followed by a colonoscopy.
Cells slough from the epithelial lining of the GI tract and pass in the stool daily. Exfoliated neoplastic cells harboring genetic alterations from tumors may be detected in stool by stool DNA testing. Currently, 1 stool DNA test is commercially available, Cologuard (Exact Sciences). It combines a FIT with an assay for a variety of genetic alterations known to be associated with colorectal neoplasia. In the hallmark trial comparing the stool DNA–FIT test with FIT using colonoscopy as the gold standard, the accuracy of a one-time stool DNA–FIT test for CRC was 92.3% versus FIT at 73.8%. The sensitivity for the detection of advanced neoplasms with stool DNA–FIT was 42.4% and with FIT was 23.8%.31 Stool DNA–FIT detected 42.4% of patients with sessile serrated polyps 1cm or larger whereas FIT detected 5.1%. The number needed to screen to detect 1 CRC with FIT was 208, with stool DNA-FIT was 166, and with colonoscopy was154. The 2016 USPSTF endorses an option of stool DNA–FIT testing every 1 or 3 years.23 A positive test requires colonoscopy.
The FDA approved a CRC screening test in 2016 that detects circulating methylated DNA in plasma. Close to 8,000 individuals 50 and older and eligible for CRC screening in Germany and the U.S., had plasma serum drawn prior to colonoscopy. Compared with the 53 cases of CRC discovered on colonoscopy, detection with methylated plasma DNA sensitivity was 48% and specificity was 91.5%. The sensitivity was best for stage IV CRC at 77.4%, but as low as 35% for stage I CRC and 11.2 % for advanced adenomas.32 With limited evidence and a low sensitivity, the USPTF does not provide formal recommendations on serum based testing and does not list it as one of the preferred screening strategies.
Over the last decade, significant advances have occurred in computed tomography colonography (CTC) technology allowing improved detection of adenomatous polyps. No data is available to determine the impact of CTC on CRC mortality. Trials comparing CTC with colonoscopy for the detection of adenomatous polyps ≥6mm report sensitivities ranging from 73% to 98% and specificities from 89% to 91%.23 CTC is less invasive than colonoscopy, may increase CRC screening rates, does not require sedation, and may not require bowel preparation although lesion detection rates are improved with bowel preparation.33 Unfortunately, CTC is less effective in detecting SSPs. Recent data show 0.8% of patients undergoing CTC were diagnosed with 1 or more SSPs compared with 4.3% of patients undergoing colonoscopy.34 The difference was significant for flat SSPs, SSPs with dysplasia, and SSPs in the right colon. CTC every 5 years is endorsed as a screening option by the USPTF, though the task force found insufficient evidence to evaluate the harms of detecting incidental findings or radiation exposure. CTC as a CRC screening option may not be covered by insurance. Colonoscopy is required for the removal lesions detected on CTC.
Flexible sigmoidoscopy (FS) allows for visualization of the distal third of the colon. Three large European and one U.S. randomized controlled trial have recently shown that FS reduces CRC incidence and in most of the trials a decrease in CRC mortality over more than a decade of follow–up (Table 5).35-38 The USPSTF guidelines recommend the use of flexible sigmoidoscopy alone every 5 years or every 10 years coupled with yearly FIT testing. Computer prediction models show improved patient life–years saved with annual FIT combined –with flexible sigmoidoscopy every 10 years screening strategy.23
| Study | No. of participants | Age, y | Design | Median follow-up, y | Results |
|---|---|---|---|---|---|
| Atkin 201035 (UK) | 170,432 (170,038 in analysis) | 55–64 |
Offered FS vs no contact | 11.2 |
Incidence reduced by 23% and mortality by 31% in group offered FS |
| Segnan 201136 (Italy) | 34,292 (34,272 in analysis) | 55–64 |
Offered FS vs no contact | 10.2 |
Incidence reduced by 18% and mortality by 22% in group offered FS |
| Schoen 201237 (U.S.) | 154,900 | 55–74 |
FS at baseline and 3 or 5 years later vs usual care | 11.9 years |
Incidence reduced by 21% and mortality by 26% in FS group+ |
| Holme 201138 (Norway) | 100,210 (98,792 in analysis) | 50–64 |
FS or FS and FOBT vs no intervention | 7 years |
Incidence reduced by 36% and mortality by 31% |
FS = flexible sigmoidoscopy; FOBT = fecal occult blood test.
Patients with small hyperplastic polyps on FS are recommended to continue with average–risk screening recommendations.39 Patients with adenomas found on FS have an increased risk of proximal advanced neoplasia. Studies have shown that among patients with advanced distal adenomas, the prevalence of advanced proximal neoplasm is 11.5% and the relative risk of advanced proximal neoplasm is 4 for those with distal tubular adenomas and 6.7 for those with advanced distal polyps compared with those with no distal adenoma.40,41 Therefore, colonoscopy is recommended in patients with adenomas detected on FS. FS every 5 years or every 10 years with annual FIT are endorsed as screening options by the USPTF.23
Colonoscopy screening in average–risk individuals has been found to be cost effective, similar to cost effectiveness per life–year saved as cervical and breast cancer screening. While no randomized controlled trials of screening colonoscopy are available, observational data demonstrates screening colonoscopy is associated with a decreased incidence of and mortality from CRC with a durable protective benefit lasting more than 10 years.42-44 Meta–analyses of observational studies of screening colonoscopy estimate a 69% reduction in the incidence of CRC with a stronger protective benefit for distal than proximal CRC. Studies of mortality from CRC associated with colonoscopy consistently show reduced mortality of up to 68%.42 The USPSTF endorses colonoscopy every 10 years in average risk individuals.23
Quality measures have been developed in order to improve the effectiveness of colonoscopy and decrease post colonoscopy CRC (PCCRC). Also known as interval CRC, PCCRC has been reported in up to 9% of patients diagnosed with CRC who had undergone colonoscopy within the previous 3 to 5 years.45-46 The major cause of interval CRC is believed to be due to missed lesion detection. The adenoma detection rate, cecal intubation rate, withdrawal time and quality of bowel preparation are some of the established quality metrics linked to the incidence of and mortality from interval CRC and should be tracked by all colonoscopists (Table 6).47A variety of bowel preparations of differing volumes, palatability, and cost are available.48-49 Data show that patients who take at least 50% of the bowel preparation the day of the procedure (called split dosing) have improved bowel cleansing and polyp detection rates compared with those that take the preparation the day before the procedure. Several trials have demonstrated FDA approved low–volume (2L) split-dose bowel preparations are equally efficacious to the 4 L split–dose preparations. The choice of bowel preparation depends on patient comorbidities and preparation characteristics. Patients who undergo colonoscopy to the cecum but are found to have inadequate bowel preparation, defined as not adequate to detect polyps >5 mm in size, should undergo repeat colonoscopy within a year due to the high rates of undetected advanced adenomas.49
| Quality metric | Goal |
|---|---|
| Cecal intubation rate | ≥95% |
| Adenoma detection rate | 25% Females ≥ Males ≥ |
| Performed to published standards and indication documented | >80% |
| Inadequate bowel preparation | <15% |
| Average withdrawal time (negative results) | ≥6 minutes |
Data from Rex, et al.47
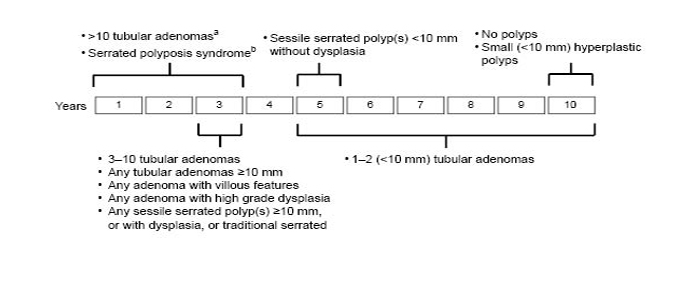
The age of onset and frequency of CRC screening and colonoscopic surveillance is dependent on personal risk factors and family history of colorectal polyps or cancer (Table 7).24 Individuals with large, numerous or histologically advanced adenomatous or serrated polyps require more frequent surveillance than individuals without such polyp characteristics (Figure 2).39 Individuals with a hereditary CRC syndrome should be recommended to undergo surveillance of the colon and extra–colonic organs at an age and frequency according to established guidelines.19-20
| Risk condition | Start screening | Screening interval |
|---|---|---|
| CRC or advanced adenomaa diagnosed in a 1st–degree relative <60 years old, OR two 1st–degree relatives of any age | The earlier of: age 40 or 10 years before the age the relative was diagnosed with CRC or advanced adenoma | 5 years |
| A 1st–degree relative ≥60 years old with CRC or advanced adenoma | Age 50 | 10 years |
| Lynch syndrome (confirmed mutation) | Age 20–25 | 2 years (age <40); 1 year (age ≥40) |
| Lynch–like syndrome or familial colorectal type | Age 20–25 | 1–2 years |
| FAP, AFAP, or MAP | Puberty | 1–2 years (1 year with established polyps) |
aAdenoma ≥1cm, with villous features, or with high–grade dysplasia.
AFAP = attenuated familial adenomatous polyposis; FAP = familial adenomatous
polyposis; MAP = MYH-associated polyposis.
Data from Rex, et al.24
Crohn's disease (CD) and ulcerative colitis are associated with an increased risk of developing CRC through the dysplasia–carcinoma pathway. Colonoscopic surveillance for dysplasia should begin 8 years following diagnosis of extensive colon involvement (above the left colon) and every 1–3 years thereafter. For disease limited to the left colon, surveillance may start 15 years after diagnosis50-51. The CRC risk is highest in individuals with long–standing ulcerative colitis with extensive disease and those with PSC. Patients diagnosed with PSC are recommended to undergo baseline colonoscopy at the time of PSC diagnosis to assess for IBD. The exam should be repeated every 1–2 years if diagnosed with IBD and every 5 years in the absence of IBD. The use of chromoendoscopy to increase the detection of visible dysplasia in lieu of random biopsies has been suggested.52 The surveillance interval, risk of CRC and surgical management of patients with dysplasia is based upon whether the dysplasia is unifocal or multi focal, visible or invisible and the completeness of resection.50, 52
Studies are mixed on the benefits and harms of utilizing vitamins, mineral or micronutrients for CRC and adenoma prevention.53-58 At present, there is no strong evidence supporting supplementation with anti–oxidants, folate, calcium, or vitamin D for the prevention of colorectal adenomas or cancer. Strong, observational data has shown benefits of long term use of aspirin in the prevention and death from CRC.59 Data from primary and secondary cardiovascular disease (CVD) prevention trials show participants receiving aspirin had a decreased 20–year CRC mortality (relative risk = 0.67) and decreased CRC incidence (relative risk = 0.60) 5 to 10 years after initiation of aspirin compared with participants receiving placebo.59 In its most recent update, the USPSTF recommends the daily use of low–dose aspirin (<100mg) for the primary prevention of CRC in adults aged 50 to 59 years old with at least a 10%, 10 year risk of a CVD.60 The appropriate patients are those not at increased risk for bleeding, have a life expectancy of at least 10 years, and are willing to take low–dose aspirin daily for at least 10 years. The decision to use aspirin in individuals ages 60 to 69 should be individualized. Other non–steroidal anti–inflammatory drugs (NSAID) such as cyclooxygenase 2 (COX–2) inhibitors have been shown in numerous trials to decrease adenoma recurrence.61-63 Unfortunately adverse cardiovascular events preclude their use for preventing colorectal neoplasia in patients with sporadic adenomas.64 A 3–year trial utilizing a combination of difluoromethylornithine and the NSAID sulindac in patients with 3 or more baseline adenomas substantially reduced adenoma and advanced adenoma recurrence.65 Numerous studies utilizing celecoxib or sulindac for colorectal polyp regression in patients with FAP have shown a reduction in polyp burden. They are often used as an adjunct to endoscopy in attenuated FAP patients with an intact colon or after colectomy for control of rectal or ileal–pouch adenomas.66-70 A randomized controlled study of patients with Lynch syndrome found a reduced incidence of CRC after 55 months in patients taking 600 mg of aspirin daily for a mean of 2 years compared with patients taking placebo.71
Most adenomas and early stage CRCs have no symptoms. Colonic blood loss is the most common sign of CRC and patients can present with a positive FOBT, iron–deficiency anemia, or hematochezia. When tumors are advanced, unexplained anorexia, weight loss, a change in bowel habits, abdominal pain, or obstruction, can occur.72 The absence of symptoms in the early stages of the disease stresses the importance of asymptomatic screening.
Invasive CRC may appear endoscopically as a tumor mass or be contained within a polyp. Surgery is curative for most early stage (TNM I–II) tumors. En bloc, completely resected malignant polyps with favorable histopathologic features may be cured with endoscopic polypectomy alone. Malignant polyps that are well differentiated, with ≥2 mm cancer-free margins, without any vascular or lymphatic invasion, and that do not penetrate through the submucosa can be managed endoscopically with favorable patient outcomes.73 Surgical management should be recommended for patients with malignant polyps with unfavorable histological features and should be considered for patients with sessile or flat malignant polyps if the patient is an appropriate surgical candidate.74
Patients with stage III (lymph node involvement) colon cancer are currently recommended to undergo postoperative adjuvant chemotherapy, which can improve overall and recurrence-free survival.75 Use of adjuvant chemotherapy in patients with stage II colon cancer may be considered in specific patients such as those with inadequately sampled lymph nodes, T4 lesions, perforation, or poorly differentiated histology. Palliative chemotherapy has a role in some patients with metastatic disease and may be combined with surgery for symptom palliation (eg, colonic obstruction or tumor bleeding) or treatment of metastatic lesions in the lung or liver.
Cancers within 12 cm from the anal verge are classified as rectal cancers. Surgical resection is curative for stage I rectal cancer. Combined therapy with surgery and perioperative chemo-radiation is recommended for most patients with stage II and III rectal cancer.76 In general, the location of the tumor within the rectum determines the technique required for excision. The goal of surgery is to perform a wide resection and a total mesorectal excision. In a total mesorectal excision, the surgeon sharply dissects along the mesorectal fascia and removes the rectum and of all the tissue invested by the adjacent visceral fascia, including fatty tissue, lymph nodes, and lymphatic vessels. Depending on the location of the tumor, the surgeon may also perform a low anterior resection or abdominoperineal resection. Tumors that involve adjacent pelvis structures require a multidisciplinary approach that includes debulking of other organs, chemotherapy or radiation or both.
Postoperative surveillance is recommended for patients treated for CRC to detect metachronous neoplasia.75,76 Surveillance colonoscopy is associated with improved overall survival though not cancer-specific survival (Table 8).77
| Cancer | Test | Surveillance interval |
|---|---|---|
| Colorectal cancer | Colonoscopy | At years 1, 3, and 5 following diagnosis. Every 5 years thereafter if normal, more frequently pending findings |
| Rectal cancer* | Endoscopic ultrasound or flexible sigmoidoscopy | Every 3–6 months for 2–3 years |
*In addition to recommendations for colonoscopy intervals.
Data from Kahi, et al.77
Gautam Mankaney, MD; nothing to disclose. Carol A. Burke, MD; nothing to disclose.