Published: September 2018
Expire: September 2021
In 1988, the International Headache Society first published a detailed classification of headache. This classification has been updated and revised multiple times, most recently in July 2013 with the publication of the International Classification of Headache Disorders, 3rd edition.1 All headaches can be classified as either a primary headache or as a secondary headache, which is defined as a headache that is caused by an underlying disease process or medical condition. Primary headache disorders are the most common. This discussion will focus on the diagnosis and management of the most common primary headaches.
Primary headache syndromes are divided into 4 groups: migraine, tension-type, trigeminal autonomic cephalalgias and other. Other is defined as headaches not of the other 3 groups that do not have a secondary cause.1 All headaches can be infrequent (episodic) or may become chronic. Chronic headache refers to a headache that occurs on 15 days or more a month. In the case of cluster headache, the most common of the trigeminal autonomic cephalalgias, chronic is defined as the absence of headache for less than 1 week a month for more than 6 months.1
Primary headaches disorders are not associated with any demonstrable structural abnormality of the brain. The diagnosis of the headache type is based on patient history, headache characteristics, and a normal neurological exam. Laboratory and imaging test results are normal, so in general, expensive studies like imaging are not obtained. During the headache attack, however, patients with cluster and migraine headache may have some abnormal clinical findings. Primary headache disorders typically occur early in life with a decreased incidence of new primary headache disorders after the age of 40 to 50.
Secondary headaches are usually of recent onset and associated with abnormalities found on clinical examination. Laboratory testing, imaging studies, or both confirm the diagnosis. Recognizing headaches related to an underlying condition or disease is critical not only because treatment of the underlying problem usually eliminates the headache, but because the condition causing the headache may be life-threatening.
Primary headaches account for more than 90% of all headache complaints, and of these, episodic tension-type headache is the most common.1 The lifetime prevalence of tension-type headache is 30% to 78% based on various studies.1,2 The mean age at onset is 25 to 30 years with a peak prevalence at 30 to 39 years. The socioeconomic impact of tension- type headache is significant.3
The prevalence of migraine varies form 12% to 20% of the population and has an estimated worldwide 1-year prevalence of greater than 1 billion.4 Migraine ranks sixth as years lived with a disability worldwide and for individuals under the age of 50, it is the third highest cause of disability.5 There are approximately 28 million migraine sufferers age 12 years and older in the United States with a prevalence of about 18% in women and 6% in males. One in 4 households has at least 1 migraine sufferer. The prevalence of migraine peaks between 25 and 55 years of age.6 Data from the Centers for Disease Control and Prevention reported the prevalence of migraine to be slightly less (8.8%) compared with diabetes (9.3%) and more prevalent than asthma (7.2%) and arthritis (5.5%).7
Cluster headache is predominant in males with a prevalence of less than 1% percent. A meta-analysis of 16 population-based epidemiologic studies found:
The pathophysiology of migraine is a complex process that begins with primary neuronal dysfunction. The dural vascular structures are innervated by neurons arising from the trigeminal nucleus and dorsal portions of the upper cervical roots. These structures project onto second order neurons in the trigeminal cervical complex and trigeminal nucleus caudalis (TNC). Fibers then ascend to the thalamus and sensory cortex. Pain is felt in the head and neck due to convergence of fibers from the trigeminal nerve via the TNC and upper cervical roots. Pain can be modulated by both descending fibers from the hypothalamus, periaqueductal grey, locus coerulus and nucleus raphe magnus onto the TNC and by ascending fibers from the hypothalamus, locus coerulus, and periaqueductal grey (Figure 1).9
Cortical spreading depression, originally only thought to occur in migraine with aura occurs in all migraines. This is a slow, self-propagating wave of cellular depolarization across the cerebral cortex that is associated with depression of neuronal activity and altered brain metabolism.10 This process also activates neurons in the TNC and causes the inflammatory process in the meningeal vascular structures to begin causing pain and headache. Brain matrix metalloproteinase is upregulated and this alters the permeability of the blood brain barrier.11
Central sensitization occurs during this process. Neurons become upregulated and sensitized to both nociceptive and non-nociceptive stimuli. This in turn causes peripheral sensitization where pain receptor fields are enlarged causing increased sensitivity to both noxious and non-noxious stimuli. Allodynia and exacerbation of pain by physical activity is thought to be caused by this process.
Although poorly understood, input from myofascial trigger points in the pericranial areas appear to be responsible for episodic tension-type headache. With prolonged nociceptive activation of the pericranial myofascia, central pain pathways are activated and may be responsible for conversion to chronic tension-type headache.12
The pathophysiology of cluster headache is poorly understood, but is believed to be caused by activation of the posterior hypothalamus with secondary activation of the trigeminal autonomic reflex through the trigeminal-hypothalamic pathway.13 Severe, unilateral pain is mediated by activation of the first division of the trigeminal nerve (V1). The autonomic symptoms associated with cluster headache (lacrimation, miosis, sweating) are thought to be due to parasympathetic outflow from the superior salivatory nucleus via the pterygopalatine (sphenopalatine) ganglion.
Headache disorders can be differentiated by type based on specific characteristics. The International Classification of Headache Disorders (ICHD), 3rd Edition is the standard by which headaches are categorized (Table 1).1
| Disorder type | Characteristics | |
|---|---|---|
| Migraine | At least 5 attacks that |
|
| Tension | At least 10 episodes of headache that last 30 minutes to 7 days associated with |
|
| Cluster | At least 5 attacks with |
|
Migraine is an episodic headache that lasts between 4 to 72 hours and fulfills the criteria established by the ICHD as shown in (Table 1).
Most patients with migraine do not have an aura, but when an aura occurs, it is defined as migraine with aura. Visual aura is most common and accounts for 90% of aura. This is typically a fortification spectra: zigzag lines that move across the visual field. Many different auras have been described: scintillating scotoma, kaleidoscope vision, pixelated vision, “orbs in the sky” to name a few. These last from 5 to 60 minutes and are followed by the headache. On occasion, these occur without headache. Sensory disturbances are the second most common aura (pins and needles sensation, numbness) usually affecting the face and arm. Language disturbance (aphasia) is unusual as is motor weakness. When motor weakness occurs, it is classified as hemiplegic migraine. When vertigo, ataxia, diplopia or other brain stem symptoms occur, it is classified as migraine with brainstem aura. Other prodromal symptoms such as yawning, irritability, neck pain, food cravings, burst of energy, or fatigue may occur hours to days preceding the migraine.
Tension-type headache is best described as a mild to moderate, featureless headache. The ICHD definition of tension-type headache is presented in (Table 1).
Cluster headache is the most common of the trigeminal autonomic cephalalgias and has been described as the “suicide” headache due to its severity. These are attacks of severe unilateral pain, occurring in and around the eye or temple and are associated with ipsilateral conjunctival injection, lacrimation, unilateral sweating, ptosis, or miosis (see Table 1 for ICHD definition). Attacks last 15 to 180 minutes, and may occur once every other day to 8 times a day. Patients are restless or agitated, and may pace or rock to try and relieve the pain. Pain often occurs 1.5 to 2 hours after the patient falls asleep, corresponding to the onset of the first REM cycle of sleep. Attacks often occur in patterns: spring and fall, around the time of the equinoxes. This is thought to be related to circadian rhythm. Alcohol is a potent trigger of the headache when a patient is in a cluster headache cycle. It does not trigger an attack outside of a cluster cycle.
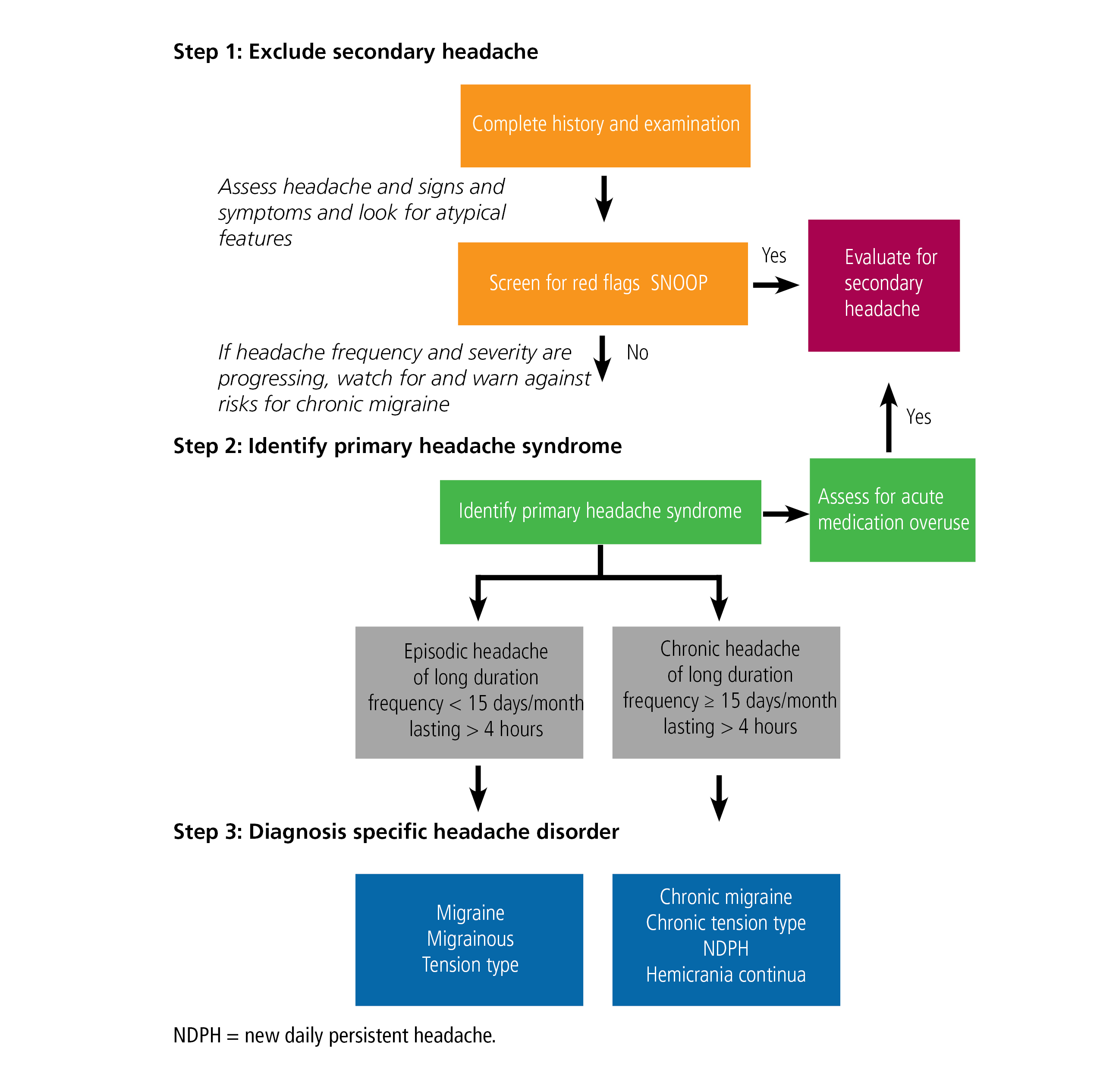
The steps to headache diagnosis are presented in (Figure 2). The first step is to always exclude a secondary headache. Excluding a secondary headache may require a laboratory evaluation or imaging or both.
The SNOOP mnemonic is useful to identify secondary headache:
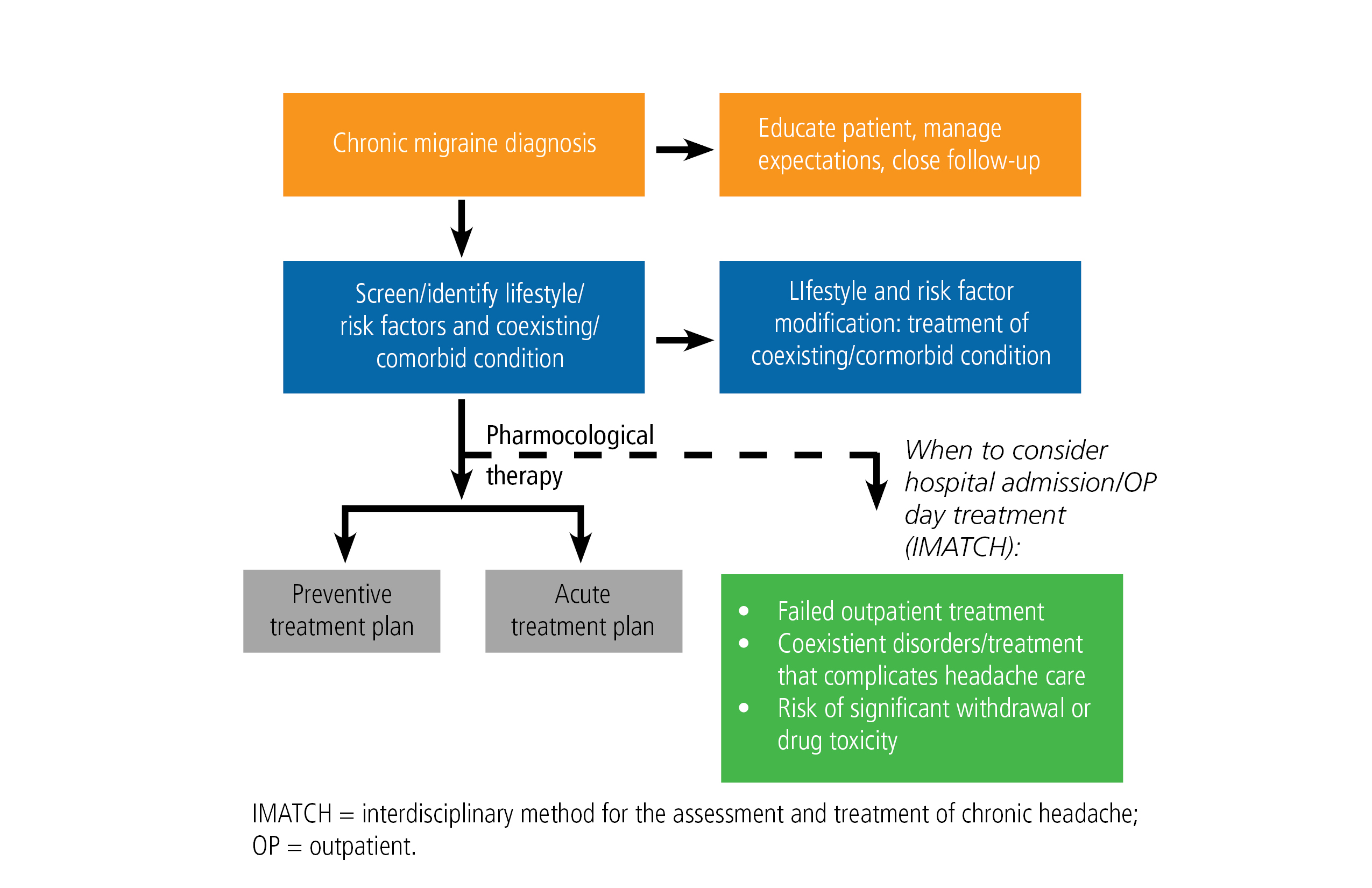
Educating the patient on migraine and its management is crucial for effective treatment. Treatment is usually a combination of general preventative measures, prophylactic treatment, and abortive treatment (Figure 3).
General preventative measures include maintaining a headache diary to identify and avoid triggers, limiting use of acute treatments (over-the-counter medications, triptans, etc.) to no more than 2 days per week or 10 days per month to prevent medication overuse headache (rebound headache), following a regular schedule (including weekends and holidays), not skipping meals, eating a balanced diet, getting 8 hours of sleep nightly, minimizing stress, exercising 30 minutes per day, keeping hydrated and drinking 6 to 8 glasses of water daily.
Goals for abortive treatment of acute migraine were published in 2000 by the US Headache Consortium and include
Always treat early in the attack before the headache progresses in severity. Whenever possible use migraine-specific medications such as triptans or dihydroergotamine. Contraindications are uncontrolled hypertension, cardiovascular and cerebrovascular disease. Use a formulation based on migraine characteristics: nasal spray or subcutaneous formulation in someone with rapid onset headache or who has nausea and vomiting from the onset. Nonsteroidal anti-inflammatory drugs (NSAIDS) are useful alternatives when triptans are contraindicated. Avoid opioids and butalbital containing compounds since these are not only addictive, but rapidly cause medication overuse headache (MOH). Do not use abortive medications more than 10 days per month to avoid MOH.
The following are the currently available triptan formulations.16
There are several reasons to consider daily medication to prevent migraines should. Prophylaxis should always be used when migraine significantly interferes with an individual’s daily routine, despite acute treatment or if the frequency of attacks are more than 1 a week. Certain uncommon migraine conditions, such as hemiplegic migraine, always require preventative treatment.
A clinic-based study on the development of chronic daily headache (CDH) over the course of 1 year showed that the risk of developing chronic daily headache increased dramatically with the frequency of migraine. The odds ratios for developing CHD was 6.2 (95% confidence interval [CI] 1.7–26.6) for patients with headache 10 to 14 days a month compared with patients with headache 0 to 4 days per month.17
The 2000 US Headache Consortium suggested daily prevention when migraine significantly interferes with the patient’s daily routine despite acute treatment, ≥ 2 long, significantly disabling attacks/month, infrequent attacks but producing profound disability, and failure, contraindication, or troublesome side effects from acute medication.15
Always start with a low dose of medication and increase gradually to minimize side effects. An adequate trial duration of therapy is 6 to 8 weeks at the target dose. Manage patient expectations because there is no quick fix and the goal of prevention is a 50% reduction in intensity or frequency or both. Encourage patients to use a calendar to accurately assess treatment benefits and evaluate efficacy. Taper the medication and discontinue it if headaches are well controlled. Instruct women about the need for birth control as many of migraine drugs are contraindicated in pregnancy. Always consider a patient’s comorbid and coexistent illnesses and disorders. One medication may be able to be used to treat concurrent disorders (Table 2).
| Drug | Contraindications | Coexisting conditions |
|---|---|---|
| Valproate | Liver disease, bleeding disorders | Epilepsy, mania, anxiety |
| Topiramate | Kidney stones | Epilepsy, mania, obesity |
| Tricyclic antidepressants (amitriptyline) | Mania, urinary retention, heart block | Other pain disorders, fibromyalgia, depression, anxiety, insomnia |
| Serotonin and norepinephrine reuptake inhibitors (venlafaxine) | Mania | Depression, fibromyalgia |
| Beta blockers | Asthma, depression, Raynaud’s diabetes, congestive heart failure | Hypertension, angina |
| Calcium channel blockers | Constipation, hypotension | Migraine with aura, hypertension, angina |
| Natural supplements | Patient preference | |
Selection of a migraine preventative drug for use should be based on clinical evidence. The American Academy of Neurology recommends evidence-based treatment for episodic migraine.18,19
Level A
Level B
aFDA approved.
The only medication specifically developed for the treatment of migraine is erenumab-aooe (Aimovig). Currently, there are 3 additional drugs targeting the calcitonin gene-related peptide receptor in phase 3 clinical trials (fremanezumab, NCT03308968; galcanezumab NCT03559257; eptinezumab).
Management of tension-type headache begins by identifying and managing possible triggers and comorbid conditions.
Analgesics such as acetaminophen and NSAIDs are usually considered to be first-line treatment for acute tension headache episodes. Combination analgesics, which combine caffeine with first-line drugs should be used as an option if analgesics alone are inadequate. Avoid use of barbiturate and opioid medications due to abuse potential and risk of MOH. Always limit use of medication to no more than 2 days a week or 10 days a month to avoid MOH. If tension headache occurs more frequently, prophylactic medication or alternative management strategies such as cognitive behavioral therapy, physical therapy, or acupuncture may be employed.
In general starting with a low dose of medicine and slowly titrating to an effective dose is the best strategy for success. Always use the smallest dose of medication necessary to prevent the headache. Tricyclic antidepressants, such as amitriptyline or nortriptyline, are first-line therapy. Serotonin and norepinephrine reuptake inhibitors, such as venlafaxine, may be used as an alternative therapy.
The main goals for management of cluster headache are to resolve the attack quickly and induce rapid remission of the episode. Management is always done concurrently with both abortive and preventative medications. Rapid control of a cluster headache cycle with a bridge between abortive and preventative medications can be done in a number of ways.
Occipital nerve blocks involve the injection of a steroid with local anesthetic into the occipital nerves. Greater occipital nerve block is done ipsilateral to the attack using either betamethasone or triamcinolone with bupivacaine 0.5%. A study by Ambrosini et al,20 found 85% (11/13) of patients with cluster headache injected with lidocaine + betamethasone were attack free at 1 week compared with patients injected with lidocaine + saline (n = 10) reporting no freedom from pain. At 4 weeks, 61% (3/13) of patients given lidocaine + betamethasone had sustained headache relief compared with no relief for patients in the lidocaine + saline group.
High-dose systemic steroids can be given over a course of 10 days to 2 weeks. Either prednisone 60 mg to 80 mg or dexamethasone should be used. A Medrol dose pack does not provide a high enough dose or a long enough duration to be of benefit.
Dihydroergotamine using a modified Raskin protocol21 can be done on an outpatient basis. The patient can be taught how to give a self-injection or the use of nasal spray to administer 1 mg every 8 hours for 3 to 5 days.
Abortive therapy for cluster headache includes high-flow oxygen (10 to 15 L/min) via rebreather mask for 15 minutes, subcutaneous dihydroergotamine or sumatriptan, or zolmitriptan 5 mg nasal spray. The oral agents work too slowly to be of benefit to abort a cluster headache.
Preventive treatment for cluster headache is with verapamil 80 mg 3 times daily to 160 mg 3 times daily. Higher doses may be necessary and an electrocardiogram should be done prior to dose escalation above 240 mg per day because of QTC prolongation. The addition of valproate or topiramate to verapamil is sometimes necessary. For chronic cluster headache, lithium is also used. Thyroid function should be monitored for patients taking lithium.
The important components of headache management include: